
UNITED STATES
CONSUMER PRODUCT SAFETY COMMISSION
4330 EAST WEST HIGHWAY
BETHESDA, MD 20814
CPSC Hotline: 1-800-638-CPSC(2772) CPSC's Web Site: http://www.cpsc.gov
Page 1 of 2
DATE:
BALLOT VOTE SHEET
TO:
The Commission
Alberta E. Mills, Secretary
THROUGH:
Patricia M. Hanz, General Counsel
Mary T. Boyle, Executive Director
FROM:
Patricia M. Pollitzer, Assistant General Counsel
Hyun S. Kim, Attorney, OGC
SUBJECT:
Draft Notice of Availability: Table Saw Blade-Contact Injuries Special Study
Report, 2017
BALLOT VOTE DUE: ____________________
CPSC staff has completed the report titled, Table Saw Blade-Contact Injuries Special
Study Report, 2017. The Office of the General Counsel has prepared a draft Federal Register
notice of availability (NOA) for the Commission’s consideration. The draft NOA announces the
availability of the report and asks for public comment on the report.
Please indicate your vote on the following options:
I. Approve publication of the attached NOA in the Federal Register, as
drafted.
(Signature)
(Date)
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
This document has been electronically
approved and signed.
November 14, 2018
Tuesday, November 20, 2018

Page 2 of 2
II. Approve publication of the attached NOA in the Federal Register, with changes. (Please
specify changes.)
(Signature)
(Date)
III. Do not approve publication of the attached NOA in the Federal Register.
(Signature)
(Date)
IV. Take other action. (Please specify.)
(Signature)
(Date)
Attachment: Draft Federal Register Notice: Notice of availability: Table Saw Blade-Contact
Injuries Special Study Report, 2017
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

DRAFT
1
[Billing Code 6355-01-P]
CONSUMER PRODUCT SAFETY COMMISSION
Notice of Availability: Table Saw Blade-Contact Injuries Special Study Report, 2017
[Docket No. CPSC-2011-0074]
AGENCY: U.S. Consumer Product Safety Commission.
ACTION: Notice of availability.
SUMMARY: The Consumer Product Safety Commission (CPSC) is announcing the
availability of a report titled, “Table Saw Blade-Contact Injuries Special Study Report,
2017.” The CPSC requests comments on the report.
DATES: Submit comments by [Insert date 60 days after date of publication in the
Federal Register].
ADDRESSES: You may submit comments, identified by Docket No. CPSC-2011-0074,
by any of the following methods:
Electronic Submissions: Submit electronic comments to the Federal eRulemaking
Portal at: http://www.regulations.gov. Follow the instructions for submitting comments.
The CPSC does not accept comments submitted by electronic mail (e-mail), except
through www.regulations.gov. The CPSC encourages you to submit electronic
comments by using the Federal eRulemaking Portal, as described above.
Written Submissions: Submit written submissions by mail/hand delivery/courier
to: Division of the Secretariat, Consumer Product Safety Commission, Room 820, 4330
East West Highway, Bethesda, MD 20814; telephone (301) 504-7923.

DRAFT
2
Instructions: All submissions received must include the agency name and docket
number for this notice. All comments received may be posted without change, including
any personal identifiers, contact information, or other personal information provided, to:
http://www.regulations.gov. Do not submit confidential business information, trade
secret information, or other sensitive or protected information that you do not want to be
available to the public. If furnished at all, such information should be submitted in
writing.
Docket: For access to the docket to read background documents or comments
received, go to: http://www.regulations.gov, and insert the docket number CPSC-2011-
0074, into the “Search” box, and follow the prompts.
FOR FURTHER INFORMATION CONTACT: Caroleene Paul, Directorate
for Engineering Sciences, U.S. Consumer Product Safety Commission, 5 Research Place,
Rockville, MD 20850; telephone: 301-987-2225; email: cpaul@cpsc.gov.
SUPPLEMENTARY INFORMATION:
On May 12, 2017, the CPSC published in the Federal Register a notice of
proposed rulemaking (NPR) on a safety standard for table saw blade-contact injuries. 82
FR 22190. In January 2017, staff began collecting additional information on incident
data identified in the National Electronic Injury Surveillance System (NEISS) for table
saws to: (1) obtain information regarding the type of table saws involved in the cases to
generate national estimates by saw type and estimated risk of injury associated with each
table saw type; (2) gain information regarding the type and usage pattern of the blade
guard; and (3) collect additional injury and incident data.

DRAFT
3
On April 27, 2017, the Commission held a decisional hearing on the NPR. The
Commission directed “staff to analyze and seek public comment on the Table Saw Study
started in January 2017, based on the most appropriate time period that will generate
information to determine a national estimate from NEISS incidents. Results will be
published in the Federal Register for notice and comment as part of the docket for this
rulemaking.”
CPSC staff has completed the report titled, Table Saw Blade-Contact Injuries
Special Study Report, 2017. The report is available on the CPSC’s website at:
_________________, and in http://www.regulations.gov, under Supporting and Related
Materials, docket number CPSC-2011-0074, and from the CPSC’s Division of the
Secretariat, at the location listed in the ADDRESSES section of this notice.
The CPSC invites comments on the report. Comments should be submitted by
[Insert date 60 days after date of publication in the Federal Register]. Information on
how to submit comments can be found in the ADDRESSES section of this notice.
Dated: _________
_____________________________________
Alberta E. Mills, Secretary
Consumer Product Safety Commission

UNITED STATES
CONSUMER PRODUCT SAFETY COMMISSION
4330 EAST WEST HIGHWAY
BETHESDA, MD 20814
Memorandum
1
Date: November 13, 2018
TO :
The Commission
Alberta E. Mills, Secretary
THROUGH:
Mary T. Boyle, Executive Director
Patricia M. Hanz, General Counsel
FROM:
George A. Borlase, Ph.D., P.E., Assistant Executive Director
Office of Hazard Identification and Reduction
Caroleene Paul, Table Saw Project Manager
Division of Mechanical and Combustion Engineering, Directorate for
Engineering Sciences
SUBJECT:
The 2017 NEISS Table Saw Special Study
1
This briefing package contains the results of the 2017 NEISS special study for table saw blade-
contact injuries. There are three tabs summarizing the study’s results:
Tab A: Garland, S. and Tu, Y. Table Saw Blade-Contact Injuries Special Study Report, 2017.
U.S. Consumer Product Safety Commission, November 2018.
In this report, Directorate for Epidemiology staff summarizes the 2017 Table Saw Special
Study’s background, design, and the methodology to generate national emergency department-
treated, table saw blade-contact, injury estimates. It also provides the response rates, reports the
national injury estimates and risk estimates, and contains results of a case-level analysis
completed by staff.
Tab B: Goldsmith, J. Table saw blade-contact injuries. Memorandum, U.S. Consumer Product
Safety Commission, November, 13, 2018.
In this memorandum, Directorate for Health Sciences staff discusses the findings of the analysis
of the 2017 NEISS data in terms of the injury diagnoses and provides the reasoning for the
review team’s decision to change injury diagnoses in some cases to characterize more accurately
the injuries sustained.
1
This analysis was prepared by CPSC staff. It has not been reviewed or approved by, and may not necessarily
reflect the views of, the Commission.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
This document has been electronically
approved and signed.

2
Tab C: Bailey, M. Table Saw Population Estimates for 2017. Memorandum, U.S. Consumer
Product Safety Commission, November 13, 2018.
In this memorandum, Directorate for Economic Analysis staff provides estimates of the number
of table saws in use in 2017 and estimates the proportion that were equipped with the modular
blade guards required under the 7
th
edition of UL 987. This memorandum presents an overview
of the data used in the analysis and describes the methodology and results of the analysis.
Additionally, an appendix presents an analysis evaluating the sensitivity of the risk findings
developed by the Directorate for Epidemiology to possible variations in the estimated proportion
of table saws equipped with the modular blade guard systems.
Recommendation
CPSC staff recommends publishing a Federal Register notice indicating the availability of the
study results (i.e., this briefing package) on CPSC.gov with a 60-day public comment period.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
3
Tab A
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

4
Table Saw Blade-Contact Injuries
Special Study Report, 2017
November 2018
Sarah Garland, Ph.D.
Yongling Tu, M.S.
Directorate of Epidemiology
Division of Hazard Analysis
U.S. Consumer Product Safety Commission
4330 East West Highway
Bethesda, MD 20814
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

5
I.
Executive Summary
In January 2017, CPSC staff initiated a special study to obtain emergency department-treated, table saw
blade-contact injury estimates for saw, incident, and injury characteristics, which are otherwise not
available in the standard NEISS data collections. In April 2017, the Commission directed staff to publish
the results for comment after the study’s completion and analysis. This report provides the results of
this study.
Study Response Rates
• For the product codes 0841 (table saws), 0845 (saws, not specified), and 0895 (power saws,
other or not specified), there were 1,342 cases identified in the NEISS, with treatment dates
between January 1, 2017 and December 31, 2017, and with a final weight greater than zero.
2
o There were 202 cases from “non-participating” hospitals. Because non-participating
hospitals do not provide patient identification, staff excluded these hospitals’ case from
follow-up investigations.
3
o For the eligible 1,140 cases from “participating hospitals”:
246 cases did not have to be assigned because the NEISS narrative indicated
that a table saw was not involved or blade contact did not occur;
128 cases did not provide victim contact information;
CPSC Field staff terminated 476 cases where no patient contact was made, the
victim refused to participate, or the case did not meet study criteria; and
Field staff completed investigations for 290 cases.
• The overall response rate for the entire study was 39.9 percent.
• For the cases where CPSC staff requested In-Depth Investigations (IDIs) to be attempted, the
response rate was 32.4 percent.
• Of the 290 completed IDIs, 161 involved a table saw blade-contact injury.
Estimated Table Saw Blade-Contact Injuries, 2017
• In 2017, there were an estimated 26,500 table saw blade-contact, emergency department-
treated injuries, with a 95 percent confidence interval of 25,200–27,800.
• Of the estimated 26,500 table saw blade-contact injuries, the table saw type distribution is:
o bench saws were an estimated 60.7 percent of the injuries (16,100);
o contractor saws were an estimated 26.6 percent of the injuries (7,000); and
o cabinet saws were an estimated 9.2 percent of the injuries (2,400).
• Of the estimated 26,500 table saw blade-contact injuries, the blade guard use distribution is:
o the blade guard was not in use in an estimated 88.9 percent of injuries (23,600);
o the blade guard was in use in an estimated 6.3 percent of injuries (1,700); and
o unknown blade guard use or situations where blade guard use is not applicable were the
remaining proportion of injuries.
• Of the estimated 26,500 table saw blade-contact injuries:
o the largest estimated proportion of injuries was for the disposition of treated and
released (86.4 percent; 22,900);
o the largest estimated proportion of injuries was to males (91.9 percent; 24,400);
o the largest estimated proportion of injuries was to the finger (96.4 percent; 25,600); and
2
See “The 2017 Study Description” section for a detailed explanation of the study design.
3
A “participating hospital” is defined as an active NEISS hospital that provides patient identification, if available, on
a case-by-case basis, as requested by CPSC staff. A “non-participating hospital” is an active NEISS hospital that
never provides any patient identification to CPSC as part of their contract. See Section VI for details.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

6
o the largest estimated proportion of injuries was to the ≥61 years age group (52.5
percent; 13,900).
Diagnosis
• There were 15 completed table saw blade-contact investigations where the corresponding NEISS
diagnosis was inappropriate or incorrect (Goldsmith, 2018). The diagnoses in these cases were
changed throughout all analyses in this report.
• The NEISS diagnosis options available also presented a challenge in characterizing table saw
blade-contact injuries. The subject matter experts (SMEs) agreed to add a diagnosis of severe
laceration. The details are found in Tab B of this package (Goldsmith, 2018). In this report, the
estimated injury results are labeled as “reviewed diagnosis.”
• This report provides the estimated number of injuries and estimated proportions of the
distribution of injuries for both the NEISS diagnosis and the reviewed diagnosis (Table 10).
Risk of Estimated Table Saw Blade-Contact Injuries, 2017
• In 2017, there were an estimated 6.9 million table saws in use, which leads to the estimated risk
of 38.62 blade-contact injuries per 10,000 table saws in use (95 percent confidence interval of
36.76 to 40.47).
o The estimated number of bench saws in use is 4.0 million, which gives the estimated risk
as 40.11 bench saw blade-contact injuries per 10,000 bench saws in use.
o The estimated number of contractor saws in use is 1.4 million, which gives the
estimated risk as 50.19 contractor saw blade-contact injuries per 10,000 contractor
saws in use.
o The estimated number of cabinet saws in use is 1.4 million, which gives the estimated
risk as 16.91 cabinet saw blade-contact injuries per 10,000 cabinet saws in use.
• In 2017, the estimated number of table saws in use that conform to UL 987, 7
th
edition
(conforming saws), is 3.9 million (57 percent). The indicator of a conforming saw in this injury
study was a saw manufactured with a modular blade guard.
o The estimated number of injuries associated with a conforming table saw is 3,200,
which is 12.2 percent of the total 26,500 estimated table saw blade-contact injuries.
o Of the estimated 21,000 injuries where the type of blade guard manufactured with the
saw is known, the estimated proportion of injuries for conforming saws is 15.4 percent.
o There is a significant proportion of injuries associated with “unknown” blade guard type
as manufactured with the table saw (19.6 percent; 5,200).
o The estimated risk of blade-contact injury associated with conforming table saws is 8.19
per 10,000 conforming saws. The estimated risk of blade-contact injury with a saw
manufactured with a traditional blade guard is 60.76 per 10,000 table saws with a
traditional blade guard.
o In 2017, the estimated relative risk of a blade-contact injury is 7.19 times more on a saw
with a traditional blade guard than on saw with a modular blade guard.
Case-Level Incident Analysis
• Section IX of this report summarizes the results of 161 investigations completed by CPSC Field
staff for injury cases involving table saw blade contact, which inform the estimated injuries. A
team of CPSC SMEs reviewed each incident in the study, and coded variables regarding the
product involved, the injury, and the incident scenario.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
7
II.
Table of Contents
I. Executive Summary ............................................................................................................................... 5
II. Table of Contents .................................................................................................................................. 7
III. List of Tables ......................................................................................................................................... 7
IV. List of Figures ........................................................................................................................................ 8
V. Introduction .......................................................................................................................................... 9
VI. The 2017 Study ................................................................................................................................... 10
The 2017 Study Description .................................................................................................................... 10
Eligible Study Cases ................................................................................................................................. 11
The 2017 Study Response Rates ............................................................................................................. 12
Completed IDI Product Identification and Blade-Contact Status ........................................................... 14
VII. Estimated Emergency Department-Treated, Table Saw Blade-Contact Injuries, 2017 ...................... 15
VIII. Estimated Risk of Emergency Department-Treated, Table Saw Blade-Contact Injuries, 2017 .......... 20
IX. Case-Level Incident Analysis ............................................................................................................... 23
X. Appendix A: Estimation Methodology for a Field Staff Investigation Study of the NEISS .................. 43
XI. Appendix B: NEISS Case Assignment Process Flow ............................................................................. 50
XII. Appendix C: SME IDI Review Process and Variable Descriptions........................................................ 51
NEISS Variables ....................................................................................................................................... 51
Saw Variables .......................................................................................................................................... 52
Injury Variables ....................................................................................................................................... 54
Incident Variables ................................................................................................................................... 55
III.
List of Tables
Table 1: NEISS Product Codes for Initial Scope of Table Saw Studies ......................................................... 11
Table 2: Case Distribution for Participating (Provides Victim Contact, if Available)................................... 11
Table 3: Eligible Cases Distribution ............................................................................................................. 12
Table 4: Investigation Response Types and Results .................................................................................... 13
Table 5: Product and Scope Identification for All Completed IDIs .............................................................. 14
Table 6: Blade Contact and Scope Identification for the 180 Completed Table Saw IDIs .......................... 15
Table 7: 2017 NEISS Estimated Injuries for Product Codes 0841, 0845, 0895............................................ 16
Table 8: Estimated 2017 Emergency Department-Treated, Table Saw Blade-Contact Injuries (Level 1) ... 16
Table 9: 2017 Estimated Emergency Department-Treated Injuries by Category (Level 2) ........................ 18
Table 10: Estimated Emergency Department-Treated Injuries by Category (Level 2), Diagnosis .............. 19
Table 11: Estimated Risk of Table Saw Blade-Contact Injury by Table Saw Type, 2017 ............................. 21
Table 12: Estimated Risk of Table Saw Blade-Contact Injury by Guard Type, 2017 ................................... 22
Table 13: NEISS Variables in Table Saw Blade-Contact Injury Completed IDIs ........................................... 24
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
8
Table 14: NEISS Diagnosis Versus SME Additional Analysis of Injury Diagnosis in Table Saw Blade-Contact
Injury Completed IDIs ................................................................................................................................. 25
Table 15: Hand Injury Variables in Table Saw Blade-Contact Injury Completed IDIs ................................. 25
Table 16: Table Saw Variables in Table Saw Blade-Contact Injury Completed IDIs .................................... 26
Table 17: Table Saw Type Versus Operator’s Use Frequency of the Saw in Table Saw Blade-Contact Injury
Completed IDIs ............................................................................................................................................ 27
Table 18: Manufactured Guard Type Versus Guard Type Received By the Operator in Table Saw Blade-
Contact Injury Completed IDIs .................................................................................................................... 27
Table 19: Manufactured Guard Type Versus SME Reviewed Diagnosis in Table Saw Blade-Contact Injury
Completed IDIs ............................................................................................................................................ 28
Table 20: Blade Guard Variables in Table Saw Blade-Contact Injury Completed IDIs ................................ 29
Table 21: Guard Use by Table Saw and Guard Characteristics in Table Saw Blade-Contact Injury
Completed IDIs ............................................................................................................................................ 31
Table 22: Guard Manufactured with Saw by When the Guard Was Removed in Table Saw Blade-Contact
Injury Completed IDIs Where the Blade Guard Was Not in Use (n = 141) ................................................. 32
Table 23: Guard Manufactured with Saw by Through/Non-through Cuts in Table Saw Blade-Contact
Injury Completed IDIs Where the Blade Guard Was Not in Use (n = 141) ................................................. 33
Table 24: Incident Characteristics in Table Saw Blade-Contact Injury Completed IDIs .............................. 36
Table 25: Stock Dimensions in Table Saw Blade-Contact Injury Completed IDIs ....................................... 37
Table 26: How Blade Contact Occurred in Table Saw Blade-Contact Injury Completed IDIs ..................... 38
Table 27: Manufactured Guard Type Versus How Blade Contact Occurred (High-Level Categories) in
Table Saw Blade-Contact Injury Completed IDIs ........................................................................................ 38
Table 28: Unexpected Workpiece Movement in Table Saw Blade-Contact Injury Completed IDIs ........... 39
Table 29: Manufactured Guard Type Versus Unexpected Workpiece Movement in Table Saw Blade-
Contact Injury Completed IDIs .................................................................................................................... 39
Table 30: How Blade Contact Occurred Versus Unexpected Workpiece Movement ................................. 40
Table 31: How Blade Contact Occurred Versus Blade Guard Use in Table Saw Blade-Contact Injury
Completed IDIs ............................................................................................................................................ 40
Table 32: Circumstances Leading to Blade Contact in Table Saw Blade-Contact Injury Completed IDIs ... 42
Table 33: Bootstrap Bias Estimates for Level 1 and Level 2 Theta Estimates ............................................. 49
IV.
List of Figures
Figure 1: Saw Safety Devices by Blade Guard in Table Saw Blade-Contact Completed IDIs, when Blade
Guard Use is Applicable and Known (n=155 of the 161 cases) ................................................................... 34
Figure 2: Operator Safety Clothing/Gear in Table Saw Blade-Contact Injury Completed IDIs ................... 35
Figure 3: Circumstance for How Blade Contact Occurred in Table Saw Blade-Contact Injury Completed
IDIs .............................................................................................................................................................. 41
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

9
V.
Introduction
On April 27, 2017, the CPSC held a decisional hearing on a notice of proposed rulemaking (NPR)
regarding the safety standard for table saw blade-contact injuries. In their briefing package to the
Commission, staff provided the statistical analysis of the NEISS cases for product code 0841 (table
saws).
4
Staff also provided a history and timeline of prior statistical studies for table saw-related
injuries, and explained why staff was not relying on those prior studies for the briefing package. For the
history of table saw injury studies conducted by the CPSC, see Tab B of the NPR briefing package. CPSC
staff noted in the briefing package that the lack of injury estimates by type of saw negatively impacts the
ability of staff to complete a full benefit-cost analysis. Therefore, in addition to the table saw injury
analysis provided in staff’s NPR briefing package, Tab B, CPSC staff developed a new study based on the
NEISS and conducted by CPSC Field staff investigators. CPSC staff called this study the 2017 NEISS Table
Saw Special Study (2017 Study). The goals of the study were: (1) to obtain information regarding the
type of table saws involved in the cases to generate national estimates by saw type and the estimated
risk of injury associated with each table saw type, (2) to gain information regarding the type and usage
pattern of the blade guard, and (3) to collect additional injury and incident details. The study began in
January 2017. At the public hearing on April 27, 2017, the Commission directed staff to completed the
study and provide a notice in the FR.
This report summarizes the 2017 Study’s design and the methodology developed by staff to generate
national estimates; it provides the response rates, and it reports the national estimates and risk
estimates, as indicated in the goals above.
Although this report summarizes the statistical results from the 2017 Study, another dimension of the
information collected in the study is the specific data regarding the injuries for table saw blade contact.
Thus, included as part of the results of this 2017 Study is an injury analysis completed by CPSC’s
Directorate for Health Sciences (Goldsmith, 2018). For risk estimates, CPSC’s Directorate for Economic
Analysis completed an analysis of estimated table saw in use (Bailey, 2018), which is provided as part of
the results of this analysis.
4
https://cpsc.gov/s3fs-public/Proposed%20Rule%20-%20Safety%20Standard%20for%20Blade-
Contact%20Injuries%20on%20Table%20Saws%20-%20January%2017%202017.pdf
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

10
VI.
The 2017 Study
The 2017 Study Description
The NEISS is a national stratified probability sample of hospitals in the United States and its territories.
There are five strata in the NEISS: children’s hospitals, small hospitals, medium hospitals, large hospitals,
and very large hospitals. Within each stratum is a sample of hospitals that makes up the primary
sampling units (PSUs) of the NEISS. For each hospital in the sample, every emergency department visit
that is associated with a consumer product is recorded. To facilitate injury estimates associated with a
product or product group, each injury has a product code that identifies the type of product involved,
and weight (i.e., the inverse of the probably of selection, adjusted for any nonresponse), which gives the
numerical representation of each case to the number of people that that case represents. Other
product-specific information, such as the name of the manufacturer, is not recorded in the NEISS.
Information recorded for each injury includes sex, age, diagnosis, disposition, and body part, among
other information. The information on stratum, hospital, age, and sex of the patient is known for all
observations in this study. Additional information about the NEISS can be found online at:
http://www.cpsc.gov/library/neiss.html
.
When resources allow, follow-up special studies are performed based on the NEISS data collected.
These special studies are often focused on a product or group of products and are used to gather more
specific information about the product(s) involved and the hazard scenario surrounding incidents.
Almost all recent special studies have used computer-assisted telephone interview (CATI) surveys to
collect information about the incident from the patient, or someone closely associated with the patient
with knowledge of the incident, such as a family member. However, due to table saw data-collection
issues documented previously, which included significant interviewer effects in several questions from
the survey,
5
in January 2017, CPSC staff began a NEISS special study collecting additional incident data
from CPSC field staff IDIs for in-scope table saw cases treated in hospitals in the year 2017, instead of
using formal survey data collection methods. This is the 2017 Study that is the subject of this report.
Appendix C describes the SME review process and final analytic data set obtained from the 2017 Study
for the set of table saw completed IDIs.
There is a product code for table saws specifically in the NEISS (0841); however, hospital coders can only
use this code if the patient used the words “table saw,” and the words “table saw” were recorded in the
hospital record. If a less-specific description is used, then a less-specific product code is used: either
0845 (saws, not specified), or 0895 (power saws, other or not specified). Cases using the less-specific
product codes (0845 and 0895) could include table saws, although the proportion of table saw cases
may be small. Nevertheless, all cases required review or investigation to discover whether the case
involved a table saw and met the study’s design requirements for the goal of obtaining accurate
estimates of table saw blade-contact injuries. Thus, staff set the initial scope of the study to review all
cases with the product codes 0841, 0845, and 0895. This covered 1,342 cases for treatment dates
January 1, 2017 through December 31, 2017, with final weight greater than zero.
5
https://cpsc.gov/s3fs-public/Proposed%20Rule%20-%20Safety%20Standard%20for%20Blade-
Contact%20Injuries%20on%20Table%20Saws%20-%20January%2017%202017.pdf (Tab B)
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
11
Eligible Study Cases
Weekly during the study, CPSC staff reviewed incoming cases from the hospitals in the NEISS with the
product codes 0841 (table saws), 0845 (saws, not specified), and 0895 (power saws, other or not
specified), to determine whether a follow-up investigation was applicable for the case, based on the
study criteria (the case from a “participating hospital” could have involved table saw blade contact). If
staff determined a case met the study criteria for a follow-up investigation, staff submitted the
investigation request and the process of obtaining patient identification from the treating hospital
began. This section summarizes the results of this process.
Altogether, there were 1,342 cases identified in the NEISS, with treatment dates between January 1,
2017 and December 31, 2017; product codes of 0841 (table saws), 0845 (saws, not specified), or 0895
(power saws, other or not specified); and with a final weight greater than zero. Table 1 provides the
product code breakdown for the initial set of cases with at least one of the three product codes in the
2017 treatment timeframe.
Table 1: NEISS Product Codes for Initial Scope of Table Saw Studies
Product Code
Number of Cases*
0841 (Table Saws)
691
0845 (Saws, not specified)
300
0895 (Power Saws, other or not specified)
351
Total
1,342
*
There were two cases in the study period that were associated with both product code 0841 and 0895; these two
cases are counted in the 0841 product code category only in this table.
Not all of the 1,342 cases were considered eligible for an IDI, although they all inform the study results
in some manner (Appendix A). Not all of the NEISS hospitals participate in providing contact information
for cases they have submitted. Accordingly, cases from non-participating hospitals had to be removed
as eligible study cases because CPSC cannot follow up where no contact information is provided. There
were 202 cases from these non-participating hospitals (Table 2); thus, 202 cases were excluded from the
possibility of a follow-up investigation.
Table 2: Case Distribution for Participating (Provides Victim Contact, if Available)
Versus Non-Participating NEISS Hospitals
Case from a Participating Hospital
Number of Cases
No
202
Yes
1,140
Total
1,342
Once the cases from non-participating hospitals were removed, CPSC staff reviewed the remaining 1,140
cases and did not assign for follow-up investigation those that were clearly not table saw injuries or
were clearly injuries not resulting from table saw blade contact.
6
CPSC staff completed this step by
reviewing, weekly for the entire year, a total of 1,140 NEISS cases and removing any cases that
6
Due to the increase in resources required for a Field staff investigation-based study compared to a CATI-based
study, where all cases would be assigned for further data collection, CPSC staff did not request investigations for
these cases. However, the non-assigned cases play an integral role in the analysis methodology; see Appendices A
and B for details.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

12
indicated, or for which staff could assume reasonably, that a table saw was not involved (e.g., cases
indicating the victim was trimming a tree) or where no blade contact occurred (e.g., corneal abrasions
due to debris while using a table saw). This left 894 cases eligible for investigation assignment requests
(Table 3); that is, 894 cases that came from a hospital that could provide contact information, if
available, and the emergency department visit could be from a table saw blade-contact incident, which
qualifies the case for a follow-up investigation to gather more specific, objective product information.
CPSC staff submitted requests for CPSC Field staff investigations on a weekly schedule throughout the
study.
Table 3: Eligible Cases Distribution
Case Eligible for Assignment
(based on staff case review)
Number of Cases
No
246
Yes
894
Total 1,140
The 2017 Study Response Rates
Table 4 provides the number of cases and percentage of cases for each type of response available in the
2017 Study, for all 1,342 cases for product codes 0841 (table saws), 0845 (saws, not specified), and 0895
(power saws, other or not specified), with a final NEISS weight greater than zero. As discussed in the
previous section, not all cases were eligible for follow-up investigation, although these cases inform the
final analysis of the study, as part of the denominator of the level 1 correction factor as cases that did
not involve table saw blade contact. Because the NEISS design captures only the first emergency
department visit for each incident and patient, duplicate cases (i.e., re-visits for the same patient and
incident) are considered out of scope for the NEISS and removed from the analyses altogether.
However, two cases involved the same victim, but for two separate incidents. Both of these cases are
in-scope for the study; CPSC Field staff completed only one IDI for both incidents (each incident is listed
separately within the IDI). There are two unique identifiers in the NEISS representing each incident, but
only one identifier for the IDI associated with these two cases. Each NEISS case is considered a
“completed IDI” in Table 4. The final total case count is 1,342 with 290 completed IDIs.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

13
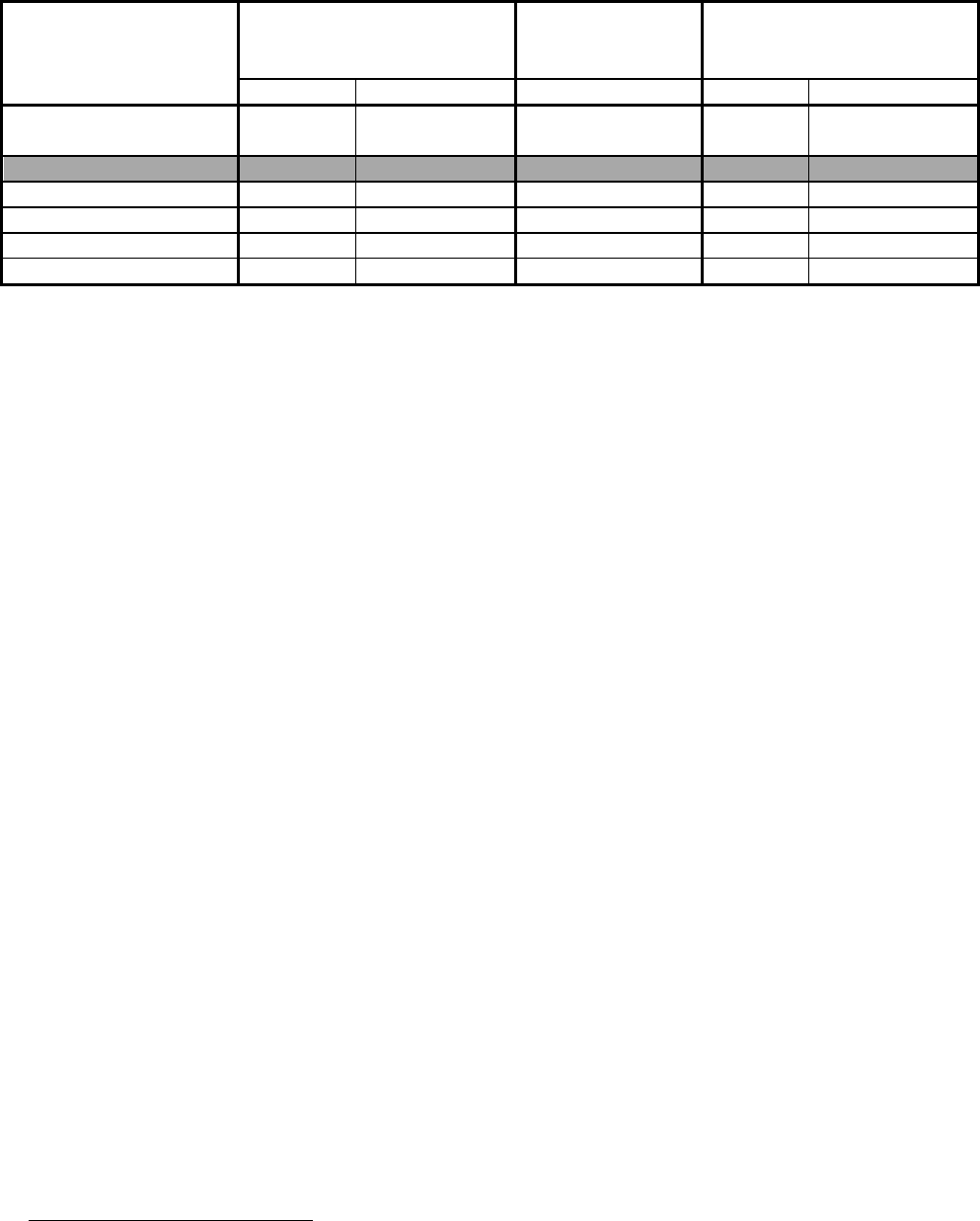
Table 4: Investigation Response Types and Results
Status
Number of Cases
Percent of Total
7
Nonresponses
Non-participating hospital 202 15%
No patient contact information available
128
10%
Terminated by Field staff
467
35%
Completed IDI, but count as nonresponse
8
9
1%
Responses
Not a table saw; Unknown if table saw, but no
blade contact; or Table saw, but no blade contact
(not assigned for investigation)
246 18%
Completed IDI 290 22%
Total
1,342
100%
For the 1,140 investigation-eligible cases, 246 cases did not have to be assigned because the NEISS
narrative regarding the incident indicated that a table saw was not involved or blade contact did not
occur. The 246 non-assigned cases are counted as responses because they are used within the analytic
methodology to answer part of the study’s overall questions. There were 128 cases without victim
contact information available from participating hospitals. Field staff terminated 467 cases when they
were unable to make contact with the patient, the victim refused to participate, or was unable to meet
study criteria (e.g., instructions to investigators included a description of when one could justify a
termination even with patient contact, because the required information would be unattainable in some
scenarios; for example, when the contact is hostile and no information that is of interest to the study is
obtained during contact).
9
In two of the terminated cases, the cases were received by CPSC staff after
the study’s data cut-off deadline, but were determined eligible for assignment. Thus, CPSC staff
classified these two cases in the “Terminated” category, although they were not assigned to the Field.
Field staff completed investigations for 290 cases. Thus, the overall response rate for the entire study
was 39.9 percent.
10
Of the 894 cases that were assigned for investigation, the hospital could not provide contact information
in 128; Field staff terminated 467 investigations and completed 290 investigations. Thus, for the cases
where CPSC staff requested that investigations be attempted, the response rate for cases with
investigations requested was 32.4 percent.
11
7
Throughout all tables of this this report, percentages may not sum to 100 percent, due to rounding.
8
There were nine completed IDIs that the SME review team marked as a nonresponse, due to the incorrect set of
questions being asked of a victim, the inability to ask most questions of the victim (e.g., a highly reluctant
respondent who essentially refused to participate, and extremely limited information gained), or other similar
circumstances. Thus, these nine IDIs did not meet the study criteria, and these nine cases are included in the
nonresponse category.
9
Unit nonresponse occurs when a case is from a hospital that does not participate in providing victim
identification, no contact was established, victim’s participation refusal, or the study’s criteria is not met.
10
( 1) =
=
= 39.9%. This corresponds to the Level 1 estimates
in the methodology provided in Appendix A, which includes table saw blade-contact estimates.
11
(
2
)
=
=
= 32.4%. This corresponds to the Level 2
estimates in the methodology provided in Appendix A, which includes table saw type estimates.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

14
Completed IDI Product Identification and Blade-Contact Status
As previously noted, the study’s goals include obtaining additional table saw blade-contact injury
information and extrapolating the data to generate national estimates. The study was initiated with a
broader scope from which one can extrapolate to the specific scope of table saw blade-contact injuries.
This section summarizes the 290 completed IDIs from the study at the product level. This section aims
to give a high-level summary of the completed investigations for the types of products identified and,
for the table saws identified, provide the blade-contact status. Detailed analyses of the table saw cases
are given throughout the remainder of this report.
Table 5 provides the products identified in the 290 completed IDIs cases. There were 180 completed
IDIs that identified a table saw as the product involved in the incident. SMEs determined that blade
contact occurred as the injury mechanism in 161 of the 180 completed IDI table saw cases (Table 6).
Table 5: Product and Scope Identification for All Completed IDIs
Product Type
Frequency
Percent of Total
Completed IDIs
Table saw
180
62.1%
Circular saw
41
14.1%
Powered miter saw/Chop saw
17
5.9%
Manual hand saw
10
3.4%
Grinder
8
2.8%
Reciprocating saw
6
2.1%
Unspecified, handheld, power saw
5
1.7%
Band saw
4
1.4%
No saw involved
4
1.4%
Jigsaw
3
1.0%
Not a table saw, but also out of scope
for the NEISS as a work-related incident
3 1.0%
Radial arm saw
2
0.7%
Biscuit joiner
1
0.3%
Chain saw
1
0.3%
Jointer
1
0.3%
Powered hedge trimmer
1
0.3%
Unspecified power saw
1
0.3%
Unspecified handheld saw
1
0.3%
Unknown saw type
1
0.3%
Total 290 100%
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

15
In calculating the Level 1 adjustment factor estimates (the estimated proportion of table saw blade-
contact injuries of the total 0841, 0845, 0895 estimated injuries), the 161 completed IDIs identified as
blade contact in Table 6 inform the numerator through the methodology described in the following
sections and in Appendix A. The denominator includes the 290 cases in Table 5, and also the 246 cases
that were not assigned (Table 4), due to scope knowledge available at the NEISS case level. These 161
cases move to inform the denominator of the Level 2 adjustment factor estimates, as described in the
following section and Appendix A, while a subset of the 161 inform the numerator, depending on the
Level 2 adjustment factor estimated under consideration.
Table 6: Blade Contact and Scope Identification for the 180 Completed Table Saw IDIs
Completed Table Saw IDI Scope
Frequency
Percent of Total
In-scope blade-contact Injury
161
89%
Not a blade-contact injury
13
7%
Out-of-scope (Occupational injury)
4
2%
Out-of-scope (Homemade table saw)
2
1%
Total
180
100%
VII.
Estimated Emergency Department-Treated, Table Saw Blade-Contact Injuries,
2017
12
Appendix A describes the full mathematical details for calculating injury estimates and associated
variance estimates for each level of incident characteristics. This section describes, more generally, the
process of obtaining injury estimates, and provides the resulting injury estimates for the year 2017.
As noted in The 2017 Study Description section, only table saw blade-contact injuries were the focus of
the study. Therefore, this study can only generate estimates specifically for blade-contact injuries for
table saws, not all injuries. However, to obtain the table saw blade-contact injury estimates, the process
is not simply taking the cases that are table saw blade-contact and summing the weights to obtain
estimates (i.e., the standard method of point estimate calculations for the NEISS). As noted in the
description in Appendix A, the methodology generates a set of adjustment factors (i.e., estimated
proportions that can be applied to a known estimate), to calculate the estimated number of emergency
department-treated injuries for a particular characteristic.
In this study, the known injury estimate (i.e., estimate derived without a special study) is all injuries
related to products in the codes 0841 (table saws), 0845 (saws, not specified), and 0895 (power saws,
other or not specified). The estimated number of injuries from these three product codes, along with
the associated variance estimated, is obtained first through the typical methodology used for obtaining
injury estimates from the NEISS. This is the top-level injury estimate that can be obtained for any year
of the NEISS, not just the special study year, given certain assumptions. In Appendix A, this estimate is
called (pronounced “tau-hat”). Adjustment factors will be applied to this estimate to obtain estimated
injuries for specific incident characteristics. Although this process can be completed for any year of the
NEISS, this section will focus on the year 2017. Table 7 provides the 2017 estimated injuries, with the 95
12
Estimates are rounded to the nearest 100 injuries. Estimated injuries may not sum to subtotal or total due to
rounding. All estimated percentages and proportions are based on unrounded estimates.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

16
percent confidence interval for the injury estimate, as obtained from the NEISS, for product codes 0841,
0845, and 0895. In 2017, there are an estimated 64,000 injuries related to products in these three
product codes (), with a 95 percent confidence interval of 55,500 to 72,400.
13
Table 7: 2017 NEISS Estimated Injuries for Product Codes 0841, 0845, 0895
Product Codes
2017 Injury
Estimate (
)
95% Confidence Interval for
the 2017 Injury Estimate (
)
0841, 0845, 0895 (All cases) 64,000 55,500 – 72,400
To obtain the estimated number of table saw blade-contact injuries, an adjustment factor is applied to
the 64,000 estimate (i.e., 64,000 is multiplied by an estimated proportion to reduce the estimate to the
measure of interest, in this case, table saw blade-contact injuries). The adjustment factor for table saw
blade-contact injuries is the Level 1 estimate,
(pronounced “theta-L-one-star-hat”), in Appendix A.
The adjustment factor calculated is 0.414, which reduces the = 64,000 estimate to 26,500, which is
called
(pronounced “phi-L-one-hat”) in Appendix A.
14
The
is 26,500, which is the estimated
number of table saw blade-contact injuries. Table 8 summarizes this process with the results.
Table 8: Estimated 2017 Emergency Department-Treated, Table Saw Blade-Contact Injuries (Level 1)
Adjustment
Factor
Estimate
95% Confidence
Interval for
2017 Injury
Estimate
95% Confidence
Interval for the 2017
Injury Estimate
0841, 0845, 0895 (All Cases)
N/A
N/A
= 64,000
55,500 – 72,400
Table saw blade-contact injuries
= 0.414
0.395 – 0.434
= 26,500
25,200 – 27,800
To obtain the estimated number of table saw blade-contact injuries for each type of table saw, along
with other characteristics of the incident, another level of adjustment factors is estimated and applied
to the estimated number of table saw blade-contact injuries that is given in Table 8. The NEISS cannot
collect information at the detailed level of the type of table saw, like a bench saw versus contractor or
cabinet saw, so estimates at this level of detail must rely on data collected through a special study. To
obtain the estimated blade-contact injuries specific for bench saws, the level 2 adjustment factor,
, is
applied to the
= 26,500, reducing this table saw blade-contact injury estimate to represent only the
bench saw blade-contact injuries. Thus, the table saw blade-contact injury estimate for any Level 2
characteristics is the estimate (the overall, unadjusted estimate for all three product codes), multiplied
by both
and
. The combination (i.e., multiplication) of these two correction factors is written as
, as a combined adjustment factor to . This process is completed for any estimate related to a detail
that can only be collected from a follow up with the patient determining further details regarding
incident and injury (Level 2 in the Appendix B flow chart). This is the
estimate in Appendix A.
Table 9 provides the estimated number of table saw blade-contact injuries for estimates for Level 2
characteristics. Level 2 estimates provided are table saw blade-contact injuries by table saw type, guard
13
All injury estimates in this report are rounded to nearest 100.
14
All adjustment factor estimates in this report are rounded to the third decimal place. However, calculations of
injury estimates and their 95% confidence intervals are based on unrounded estimates, and the results are then
rounded for this report.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
17
usage, guard type as manufactured with the saw, diagnosis, the NEISS disposition, injured body part,
victim’s age group, and victim’s sex. Though other variables the SME review team coded in the study
are considered Level 2 as well, the methodology from Appendix A is computationally intensive, so CPSC
staff limited estimates to this specific set of characteristics, which meet the main goals of the study.
Section IX provides the results of all study variables at the case level without extrapolation to national
estimates.
Part of the first goal of the 2017 Study was to provide estimated injuries by table saw type. Of the
estimated 26,500 table saw blade-contact injuries, an estimated 16,100 (60.7 percent) and 7,000 (26.6
percent) are bench and contractor saws, respectively. The remaining part of the estimated blade-
contact injuries are for cabinet saws and table saws where a type of saw cannot be determined.
Blade guard use was also another area of interest to understand as part of the 2017 Study. In 2017, of
the estimated 26,500 table saw blade-contact injuries, 23,600 (88.9 percent) occurred without a blade
guard in use, while 1,700 occurred with a blade guard in use (6.3 percent). For a more detailed case-
level analysis concerning blade guard use, see Section IX of this report.
In 2017, of the 26,500 estimated table saw blade-contact injuries, an estimated 17,800 (67.0 percent)
occurred on a saw manufactured with a traditional blade guard, while an estimated 3,200 injuries
occurred on a table saw manufactured with a modular blade guard (12.2 percent). A non-trivial
proportion (an estimated 19.6 percent or an estimated 5,200 injuries) of the estimated blade-contact
injuries occurred on a table saw where the type of blade guard manufactured with the saw could not be
determined. With this in mind, considering the estimated injuries where the blade guard type that was
manufactured with the saw was known (21,000), the majority (84.6 percent) of the estimated injuries
are for saws manufactured with a traditional blade guard, and saws manufactured with a modular blade
guard are an estimated 15.4 percent. Note that from a statistical perspective, the breakdown of the
type of blade guard by whether the blade guard is in use is not possible due to the small sample sizes;
however, this additional breakdown is provided at the case level in Section IX.
A majority of the estimated 26,500 table saw blade-contact injuries were treated and released in the
emergency department (22,900; 86.4 percent), while an estimated 11.7 percent (3,100) were
hospitalized (i.e., treated and transferred or treated and admitted).
A majority of the estimated 26,500 table saw blade-contact injuries occurred to at least one finger
(24,400; 91.9 percent) and to males (25,600; 96.4 percent).
About half of the estimated 26,500 table saw blade-contact occurred to the ≥61 age group (52.5
percent; 13,900), while the 41-60 age group and ≤40 age group had an estimated 35.1 percent and 12.4
percent of the injuries (9,300 and 3,300), respectively.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

18
Table 9: 2017 Estimated Emergency Department-Treated Injuries by Category (Level 2)
Table Saw Blade-Contact
Injuries
15
Estimate
Estimate
2017 Injury
Estimate,
95% CI for the 2017
Injury Estimate
Table Saw Type
0.607
0.252
16,100
15,300 – 16,900
Bench
Contractor
16
0.266
0.110
7,000
6,600 – 7,500
Cabinet
0.092
0.038
2,400
2,200 – 2,700
Unknown
*
*
*
*
Blade Guard Use
0.889
0.368
23,600
22,400 – 24,800
No
Yes
0.063
0.026
1,700
1,500 – 1,900
Unknown
*
*
*
*
N/A
*
*
*
*
Guard Type
Manufactured with Saw
0.670
0.278
17,800
16,800 – 18,700
Traditional
Modular
0.122
0.050
3,200
2,900 – 3,500
Unknown
0.196
0.081
5,200
4,500 – 5,900
None
*
*
*
*
Disposition
0.864
0.358
22,900
21,700 – 24,100
Treated and Released
Hospitalized
17
0.117
0.048
3,100
2,800 – 3,400
Other
*
*
*
*
Body Part
0.919
0.381
24,400
23,100 – 25,600
Finger
Hand
0.073
0.030
1,900
1,700 – 2,200
Other
*
*
*
*
Sex
0.964
0.399
25,600
24,300 – 26,800
Male
Female
*
*
*
*
Age Group
0.124
0.051
3,300
2,600 – 4,000
≤40
41-60
0.351
0.145
9,300
8,800 – 9,800
≥61
0.525
0.217
13,900
13,200 – 14,600
*Indicates an injury estimate that is considered unstable; thus, is not reported in this table.
15
There are 10 cases with completed IDIs that inform the table saw type = “Cabinet” estimate, and similarly, 10
cases for table saw type=“Unknown,” 14 cases for blade guard use = “Yes,” and 15 cases for body part = “Hand.”
Typically, this is a smaller number of cases than usual for producing a stable estimate with the NEISS; however, the
methodology applied here is not the methodology used to generate the reporting criteria for the NEISS. These
estimates otherwise meet the standard NEISS stability criteria, except for table saw type = “Unknown.” These
estimates are reported here, but with this note. However, if an estimate failed a second reporting criteria, as with
table saw type = “Unknown,” the estimate is not reported.
16
The contractor saw category includes contractor saws and hybrid table saws. See Section IX (Table 16).
17
The “Hospitalized” category includes the NEISS dispositions of admitted and transferred.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

19
In reviewing the additional information obtained through the IDIs, the SME review team determined
that the injuries sustained in these incidents were not easily captured by a single diagnosis code
available in the NEISS (See the “Case-Level Incident Analysis” section of this report and Tab B
(Goldsmith, 2018) for additional details). The injuries were, at times, severe lacerations that the NEISS
had captured through various diagnosis codes, but those single diagnosis codes did not describe the full
extent of the injuries. Additionally, the SME review team determined the NEISS diagnosis was
inappropriate or incorrect in 15 cases. Thus, the SME review team reviewed the information available
and made a determination about the NEISS injury code. This report does not go into the details of these
injuries, but refers the reader to the Directorate for Health Science’s memorandum (Tab B), which is
part of this package and provides a detailed analysis of table saw blade-contact injuries from the 2017
Study (Goldsmith, 2018). The estimated injuries for the NEISS diagnosis and the Reviewed Diagnosis (a
classification that captures more of the extent of the injury), but both incorporating the corrected value
for the 15 inappropriate or incorrect cases, are given in Table 10.
While the laceration diagnosis remained the prevalent diagnosis in table saw blade-contact injuries,
regardless of the classification method, the SME review team’s “reviewed diagnosis” captured severe
lacerations at an estimated 15.1 percent of the estimated 26,500 table saw blade-contact injuries, and
lacerations at an estimated 53.2 percent (estimates of 4,000 and 14,100, respectively). There is a
statistically significant difference between the laceration diagnosis from the NEISS diagnosis and the
reviewed diagnosis of laceration, and the severe laceration classification cannot be compared between
the two, as the severe laceration classification is unique to the 2017 Study, as described.
The amputation diagnosis represents 10.7 percent of the estimated table saw blade-contact injuries for
the NEISS diagnosis, and 13.3 percent of the reviewed diagnosis; there is not a statistically significant
difference between these two estimates. Fracture diagnoses within the NEISS diagnosis often shifted to
the severe laceration category in the reviewed diagnosis; thus, a significant change is seen in the
fracture and other classifications between NEISS diagnosis and reviewed diagnosis. An estimated 20.6
percent of the table saw blade-contact injuries within the NEISS diagnosis are fractures, while fractures
had to be combined with the avulsion diagnosis to yield statistical results in the reviewed diagnosis. See
Table 13 in Section IX for the comparison of the NEISS diagnosis to the reviewed diagnosis, and see
(Goldsmith, 2018) for a detailed analysis of the injuries in the 2017 Study.
Table 10: Estimated Emergency Department-Treated Injuries by Category (Level 2), Diagnosis
Table saw blade-contact
Injuries
18
Estimate
Estimate
2017 Injury
Estimate,
95% CI for the 2017
Injury Estimate
NEISS Diagnosis
0.609
0.252
16,100
15,200 – 17,100
Laceration
Fracture
0.206
0.085
5,500
5,100 – 5,800
Amputation
0.107
0.044
2,800
2,600 – 3,100
Other
0.078
0.032
2,100
1,800 – 2,300
Reviewed Diagnosis
0.532
0.220
14,100
13,200 – 15,000
Laceration
Severe Laceration
0.151
0.063
4,000
3,600 – 4,400
Amputation
0.133
0.055
3,500
3,200 – 3,800
Fracture or Avulsion 0.184 0.076 4,900 4,500 – 5,200
18
from Table 6 (
= 26,500).
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

20
VIII.
Estimated Risk of Emergency Department-Treated, Table Saw Blade-Contact
Injuries, 2017
In the previous section, Table 8 gives the estimated number of table saw blade-contact injuries in 2017.
Table 9 breaks down that estimate for each type of table saw, whenever it is possible. In this section,
the estimated number of injuries is divided by the estimated number of table saws in use
19
to obtain the
estimated risks of injury. Confidence intervals are also provided to understand the results.
20
Table 11 provides the estimated number of table saws in use for all table saw types and by type of table
saw.
21
This estimated number of table saws in use becomes the denominator for the risk of table saw
blade-contact injuries, which is provided as the estimated number of blade-contact injuries per 10,000
table saws in use. For all types of table saws, the estimated risk is 38.62 blade-contact injuries per
10,000 table saws in use, with a 95 percent confidence interval of 36.76 to 40.47.
Bench saws are estimated at approximately 60 percent of the total estimated number of table saws in
use, and contractor and cabinet saws comprise approximately 20 percent each. The estimated risk is
40.11 blade-contact injuries per 10,000 bench saws in use, 50.19 per 10,000 contractor saws in use, and
16.91 per 10,000 cabinet saws in use. The risk of blade-contact injury is highest for contractor saws, and
lowest for cabinet saws, with all risk comparisons being statistically different.
The proportions of the estimated number of table saws in use for bench and contractor saws (58.5
percent and 20.4 percent, respectively) is similar to the proportions of blade-contact injuries for bench
and contractor saw blade contact injuries (60.7 percent and 26.6 percent for bench and contractor saw
injuries, respectively). For cabinet saws, there is observable difference in the proportion of estimated
table saws in use (21.1% of all table saws in use) versus the proportion of blade contact injuries (9.3% of
table saw blade contact injuries).
19
The term “in use” does not refer to the frequency of use, but to the number of units available for use.
20
The variance estimate for the risk estimates are assumed to be the same as the variance for the corresponding
injury estimate. This is not likely the case in reality; however, there is not a closed form of the variance estimator
for the denominator, and it is unlikely that there would be enough of an impact on the confidence interval
calculations for any conclusions to be affected.
21
CPSC’s Directorate for Economics provided the estimated number of table saws in use for this analysis; details
are provided in (Bailey, 2018), which is Tab C of this briefing package.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
21
Table 11: Estimated Risk of Table Saw Blade-Contact Injury by Table Saw Type, 2017
Table Saw Type
2017 Injury Estimates
Estimated Number
of Saws in Use
(in 10,000’s)*
22
Risk of Table saw blade-
contact Injury per 10,000 Table
Saws in Use
Estimate
95% CI
Estimate
Estimate
95% CI
Table Saw Blade-Contact
(All Table Saw Types)
26,500 25,200 – 27,800 686.32 38.62 36.76 – 40.47
Type of Table Saw
Bench Saw
16,100
15,300 – 16,900
401.28
40.11
38.02 – 42.20
Contractor Saw
7,000
6,600 – 7,500
140.26
50.19
46.84 – 53.54
Cabinet Saw
2,400
2,200 – 2,700
144.78
16.91
15.15 – 18.67
Unknown
*
*
N/A
N/A
N/A
* See (Bailey, 2018), Tab C of this briefing package.
Table 12 considers the risk of injury for table saws in use that conform to UL 987, 7
th
edition, which
requires modular blade guards. For injuries, the assumption is that if a table saw was manufactured
with a modular blade guard, then it is conforming to UL 987, 7
th
edition (conforming saws). Although
this may not be true in 100 percent of the cases, it is a reasonable assumption. Table saws
manufactured with a traditional blade guard are nonconforming saws.
Of the estimated 686,320 table saws available for consumer use in 2017, table saws (all types)
conforming to UL 987, 7
th
edition comprise an estimated 57 percent of table saws in use. The estimated
proportion of blade-contact injuries associated with conforming table saws in 2017 is 12.2 percent
(Table 9); however, there is a significant proportion of blade-contact injuries (19.6 percent) where the
manufacturer-supplied guard type is “unknown.” Thus, considering only estimated blade-contact
injuries where blade guard type is known (21,000), an estimated 15.4 percent (3,200) of blade-contact
injuries are associated with table saws conforming to the voluntary standard, while, of course, the
proportion of table saws in use that are conforming remains at the estimated 57 percent mentioned
above.
In 2017, the estimated risk of a table saw blade-contact injury per 10,000 saws in use that were
manufactured with a traditional blade guard is 60.75, while the estimated risk of a blade-contact injury
per 10,000 modular blade guard saws is 8.19. This gives an estimated relative risk for 2017 of 7.19,
which means that the risk of injury on a saw with a traditional blade guard is about 7 times greater than
on a saw with a modular blade guard.
22
The term “in use” does not refer to the frequency of use, but to the number of units available for use.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

22
Table 12: Estimated Risk of Table Saw Blade-Contact Injury by Guard Type, 2017
Table Saw Type
2017 Injury Estimates
Estimated Number
of Saws in Use
(in 10,000’s)*
23
Risk of Table Saw Blade-
Contact Injury per 10,000
Table Saws in Use
Estimate
95% CI
Estimate
Estimate
95% CI
Table Saw Blade-Contact (All
Table Saw Types)
26,500 25,200 – 27,800 686.32 38.62 36.76 – 40.47
Type of Guard Manufactured
with Saw
Traditional
17,800
16,800 – 18,700
292.19
60.75
57.53 – 63.99
Modular
3,200
2,900 – 3,500
394.12
8.19**
7.48 – 8.90
Unknown
5,200
4,500 – 5,900
N/A
N/A
N/A
None
24
*
*
N/A
N/A
N/A
* See (Bailey, 2018), Tab C of this briefing package.
**There is a significant proportion of blade contact injuries for which the blade guard type manufactured with the
table saw is “unknown.” This should be considered in understanding the risk of blade-contact associated with
conforming versus nonconforming table saws.
23
The term “in use” does not refer to the frequency of use, but to the number of units available for use.
24
For the “None” category, the saw in this incident, there was no evidence from the investigation that the saw was
originally manufactured with a blade guard, given the saw’s age and reported information regarding the saw (see
Case-Level Incident Analysis for counts of cases for each level).
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

23
IX.
Case-Level Incident Analysis
Previous sections provide national injury estimates based on the results of the 2017 Study. As part of
the study, CPSC Field staff completed 161 investigations for injury cases involving table saw blade
contact.
25
A team of CPSC SMEs reviewed each completed IDI in the study, and the team coded
variables regarding the product involved, the injury, and the incident scenario. This section summarizes
the findings from completed IDIs associated with table saw blade-contact injuries based on the staff
review. Appendix C provides the data review and coding process, and also provides variable definitions
and categories for variables, as applicable.
The 161 completed IDIs on table saw blade-contact injuries informed the adjustment factors for the
table saw blade-contact estimates that were calculated and applied in the prior sections of this report.
This section is not intended to provide national estimates for all the characteristics of these incidents;
instead, this section provides an analysis to understand the types of incidents that have informed the
nationally representative injury estimates set forth in Sections VII and VIII of this report. Neither case
weights, nor adjustment factors, are applied in this section; all frequency and percentages reported are
at the case (anecdotal) level. Thus, the reader should not expect that the percentages presented in this
section match percentages of national estimates provided. To the contrary, the percentages in this
section most likely do not match national estimate proportions, but may be similar, or not, depending
on a number of factors.
Table 13 provides the breakdown of the 161 table saw blade-contact injury, completed IDI cases for the
variables age group, sex, diagnosis, disposition, and body part.
There were 15 cases where the NEISS diagnosis code was determined to be inappropriate or incorrect,
and these 15 cases are reflected in this analysis based on the corrected diagnosis, in both the NEISS
diagnosis variable and in the Reviewed Diagnosis variable. While the Reviewed Diagnosis variable
created a way for the review team to capture the table saw blade-contact injuries in a repeatable and
more descriptive way, these 15 cases were unique. These 15 cases were inappropriate or incorrect in
the original NEISS, and not just inadequate in their description of the injuries; thus, these 15 cases
reflect the corrected diagnosis in both the NEISS Diagnosis variable and Reviewed Diagnoses variable
(Goldsmith, 2018). Similarly, there was one case where the body part coded in the NEISS was not
correct; the body part results throughout this analysis reflect the corrected body part code for the case.
25
As noted in Section VI, there was a total of 290 completed investigations for the whole study. Of these 290
completed IDIs, 129 did not involve a table saw blade-contact injury. Of the 180 table saw completed IDIs, 19 did
not involve blade contact.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

24
Table 13: NEISS Variables in Table Saw Blade-Contact Injury Completed IDIs
Variable
Frequency
Percent of Total
Age Group
≤40
25
15.5
41-60
55
34.2
≥61
81
50.3
Sex
Male
153
95.0
Female
8
5.0
NEISS Diagnosis
Laceration
105
65.2
Amputation
19
11.8
Fracture
29
18.0
Avulsion
7
4.4
Nerve Damage
1
0.6
Disposition
Treated and Released
132
82.0
Hospitalized
26
26
16.1
Other
3
1.9
Body Part
Finger
145
90.1
Hand
15
9.3
Lower Arm
1
0.6
As described, in reviewing the additional information obtained through the IDIs, the SME review team
often determined that the injuries sustained in these incidents were not easily captured by a single
diagnosis code in the NEISS. As described in Goldsmith, 2018; section 3, provided as Tab B of this
briefing package, some of the limitations arise from the single diagnosis construct of the NEISS.
Additionally, the injuries were, at times, severe lacerations that the NEISS had captured through various
diagnosis codes, but for which no single diagnosis code was sufficient to explain the full extent of the
injuries. Thus, the SME review team reviewed the information available and made a determination
about the NEISS injury code. Table 14 shows the original NEISS diagnosis code compared to the SME
review team’s reviewed-diagnosis determinations. As mentioned previously, there were 15 cases that
the review team determined to be inappropriate or incorrect diagnosis codes in the NEISS, and the
diagnosis has been corrected throughout this analysis and report. There were 29 cases with a reviewed
diagnoses of laceration that the team determined to be an extreme severity. This report does not go
into the details of these injuries, but refers the reader to the Directorate for Health Science’s
memorandum, which is part of this package (Tab B) and provides a detailed analysis of table saw blade-
contact injuries from the 2017 Study (Goldsmith, 2018).
26
The “Hospitalized” category includes the NEISS dispositions of admitted and transferred.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

25
Table 14: NEISS Diagnosis Versus SME Additional Analysis of Injury Diagnosis in Table Saw Blade-Contact Injury
Completed IDIs
n
Row %
SME Reviewed Diagnosis
Total
NEISS Diagnosis*
Laceration
Severe Laceration
Amputation
Fracture
Avulsion
Laceration
80
76.2
22
21.0
0
0.0
2
1.9
1
1.0
105
Amputation
0
0.0
0
0.0
19
100.0
0
0.0
0
0.0
19
Fracture
5
17.2
6
20.7
5
17.2
13
44.8
0
0.0
29
Avulsion
1
14.3
0
0.0
0
0.0
0
0.0
6
85.7
7
Nerve Damage
0
0.0
1
100.0
0
0.0
0
0.0
0
0.0
1
Total
86
53.4
29
18.0
24
14.9
15
9.3
7
4.4
161
*Includes the corrected diagnosis to 15 cases, as described in the text.
Of the 161 completed IDIs that are in-scope for table saw blade-contact injuries, the operator of the
table saw was the injured person in 160 (99.4 percent) of the cases, while one case involved a bystander
or assistant. Most cases did not involve more than one person, regardless of injured party.
Table 15 shows the cross-tabulation for the victim’s dominant hand versus injured hand in the 161 table
saw blade-contact completed IDIs. In the 161 cases, 127 victims reported as right-handed (78.9 percent),
10 as left-handed (6.2 percent), and nine as ambidextrous (5.6 percent). The remaining 15 cases have
an unknown dominant hand for the victim. Of the 137 completed IDIs where the victim reported to be
left- or right-hand dominant, 91 cases involved the injury occurring to the victim’s non-dominant hand
(66.4 percent).
Table 15: Hand Injury Variables in Table Saw Blade-Contact Injury Completed IDIs
n
Row %
Injured Hand
Total
Dominant Hand
Left
Right
Unknown
Left
4
40.0
6
60.0
0
0.0
10
Right
85
66.9
42
33.1
0
0.0
127
Ambidextrous
9
100
0
0.0
0
0.0
9
Unknown
8
53.3
2
13.3
5
33.3
15
Total
106
65.8
50
31.1
5
3.1
161
Table 16 provides the distribution of the 161 table saw blade-contact injury, completed IDIs for the table
saw type, the guard type the saw was manufactured with, the guard type the operator received when
the saw was acquired, and the operator’s use frequency of the saw involved in the incident.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

26
Of the 161 table saw blade-contact injury cases, bench saws were involved in 100 cases (62.1 percent),
while contractor saws were involved in 41 cases (25.5 percent). Cabinet saws and unknown saw type
are both associated with 10 cases each (both 6.2 percent).
A table saw is expected, for the most part, to have been manufactured and sold with a blade guard, and
that blade guard will be either the traditional type or the modular type of blade guard. However, saws
not only are purchased new by consumers, but also are purchased used, given away, borrowed, passed
down, or shared by a group of users. Accordingly, the blade guard that was manufactured with the saw
does is not necessarily available for use for the operator. For the 161 table saw blade-contact injury
completed IDIs in the 2017 Study, 35 (21.7 percent) involved a situation where the operator did not
receive a blade guard when the saw was acquired for use by the operator.
Of the 161 table saw blade-contact injury completed IDI cases, the majority of operators reported using
the incident saw daily to weekly or weekly to monthly (33.5 and 27.3 percent, respectively).
Table 16: Table Saw Variables in Table Saw Blade-Contact Injury Completed IDIs
Variable
Frequency
Percent of Total
Total
161
100%
Table Saw Type
Bench
100
62.1
Contractor
27
41
25.5
Cabinet
10
6.2
Unknown
10
6.2
Guard Type Manufactured
with Saw
Traditional
102
63.4
Modular
25
15.5
None
1
0.6
Unknown
33
20.5
Guard Type Received by
Operator when Saw Acquired
Traditional
76
47.2
Modular
24
14.9
N/A-None
35
21.7
Unknown
26
16.2
Operator’s Use Frequency of
the Saw
First Time
3
1.9
Daily to Weekly
54
33.5
Weekly to Monthly
44
27.3
Monthly to Yearly
28
17.4
Yearly
5
3.1
Other
12
7.5
Unknown
15
9.3
27
Hybrid table saws account for 2 of total 41 in the “Contractor” table saw type category.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

27
Table 17 provides the breakdown of the table saw type with the operator’s frequency of use.
Contractor use frequency is distributed more towards the higher available use frequency categories,
while bench saws had a more even spread throughout the use frequencies. Cabinet saws are shifted
towards the higher use frequency categories.
Table 17: Table Saw Type Versus Operator’s Use Frequency of the Saw in Table Saw Blade-Contact Injury
Completed IDIs
n
Row %
Operator’s Use Frequency of the Saw
Total
Table Saw Type
Daily to
Weekly
Weekly to
Monthly
Monthly
to Yearly
Yearly
First
Time
Other
Unknown
Bench
29
29.0
26
26.0
21
21.0
4
4.0
2
2.0
8
8.0
10
10.0
100
Contractor
16
41.0
13
33.3
6
14.6
0
0.0
1
2.6
3
7.3
1
2.4
39
Cabinet
6
60.0
1
10.0
0
0.0
1
10.0
0
0.0
1
10.0
1
10.0
10
Unknown
2
20.0
4
40.0
1
10.0
0
0.0
0
0.0
0
0.0
3
30.0
10
Total
54
44
28
5
3
12
15
161
Table 18 gives the cross-tabulation for the manufactured guard type by the type of guard received by
the operator when the saw was acquired or used. In 20.5 percent of the 161 cases, the type of guard
manufactured with the saw was unknown; and in 16.2 percent of the cases, it was unknown if or what
type of guard was received by the operator with the saw (Table 16). Although the “Unknown” category
is a significant proportion in each, of the saws in the 102 blade-contact injury cases known to be with a
saw manufactured with a traditional blade guard, the blade guard was received with the saw at the time
of acquisition in 76 cases (74.5 percent); while in 20 cases (19.6 percent), the operator did not receive
the blade guard when the saw was acquired. In the 25 cases with saws identified as being manufactured
with a modular blade guard, in 24 cases (96.0 percent) the operator did receive the blade guard when
the saw was acquired.
Table 18: Manufactured Guard Type Versus Guard Type Received By the Operator in Table Saw Blade-Contact
Injury Completed IDIs
n
Row %
Guard Type Received by Operator
when Saw Acquired
Total
Manufactured Guard Type
Traditional
Modular
Unknown
N/A-None
Traditional
76
74.5
0
0.0
6
5.9
20
19.6
102
Modular
0
0.0
24
96.0
0
0.0
1
4.0
25
Unknown
20
60.6
0
0.0
0
0.0
13
39.4
33
None
0
0.0
0
0.0
0
0.0
1
100.0
1
Total 76 24 26 35 161
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

28
Table 19 provides the cross-tabulation of type of guard manufactured with the saw versus the SME
review team diagnosis classification, regardless of whether the blade guard was in use at the time of the
incident. Due to the small number of cases with modular blade guards, and those cases being spread
across several diagnoses, staff recommends limiting conclusions being drawn from this table. That being
said, cases for saws manufactured with a modular blade guard seem to veer towards less severe
diagnosis compared to the distribution of cases for traditional blade guard saws.
Table 19: Manufactured Guard Type Versus SME Reviewed Diagnosis in Table Saw Blade-Contact Injury
Completed IDIs
n
Row %
SME Reviewed Diagnosis
Total
Guard Type
Manufactured with Saw
Laceration
Severe
Laceration
Amputation
Fracture
Avulsion
Traditional
50
49.0
19
18.6
19
18.6
9
8.8
5
4.9
102
Modular
15
60.0
6
24.0
2
8.0
2
8.0
0
0.0
25
None
0
0.0
0
0.0
0
0.0
0
0.0
1
100.0
1
Unknown
21
63.6
4
12.1
3
9.1
4
12.1
1
3.0
33
Total
86
53.4
29
18.0
24
14.9
15
9.3
7
4.4
161
Table 20 provides the distributions for blade guard use, and for those cases where the blade guard was
not in use, the table provides a summary of why the guard was not in use and when the guard was
removed. In the 161 table saw blade-contact injury cases with completed IDIs, the majority, 141 cases
(87.6 percent), did not involve the use of a blade guard, for a variety of reasons. The most common
category (44.7 percent of the 141 cases without a blade guard in use) for blade guard removal included
reports of the blade guard being inconvenient, blocking the view of the cut, the stock size, the cut type,
or a combination of these. The second most common category was having not received a blade guard
when the saw was acquired (35 cases, 24.8 percent).
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

29
Table 20: Blade Guard Variables in Table Saw Blade-Contact Injury Completed IDIs
Variable
Frequency
Percent of Total
Blade Guard Use
Yes
14
8.7
No
141
87.6
Unknown
5
3.1
N/A
1
0.6
Total
161
100%
When was the guard removed?
(for guard in use = no)
Removed prior to the operator acquiring the saw (i.e.,
the operator did not receive a blade guard with the
saw)
35 24.8
Never installed
23
16.3
Removed for some reason after the operator acquired
the saw
50 35.5
The guard was in the up position, not removed
entirely
8 5.7
Unknown
25
17.7
Total
141
100%
Why was no guard in use?
(for guard in use = no)
Inconvenient/visibility/cut type/stock size
63
44.7
Did not receive a guard when saw acquired
35
24.8
Broken
6
4.3
Lost
2
1.4
Difficulty installing
2
1.4
Broken; Lost;
Inconvenient/visibility/cut type/stock size
1 0.7
Difficulty installing;
Inconvenient/visibility/cut type/stock size
1 0.7
Other
9
6.4
Unknown
22
15.6
Total 141 100%
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
30
Table 21 gives the cross-tabulations for blade guard use at the time of the incident versus the type of
guard manufactured with the saw, the guard type received with the saw, the table saw type, and the
SME reviewed diagnosis. The proportion of blade guards not in use for the 161 blade-contact cases is
fairly even across the type of blade guard manufactured with the saw (89.2, 88.0, and 81.8 percent for
traditional, modular, and unknown blade guard types, respectively). And similarly, for the type received,
the majority of blade guards were not in use across all blade guard type categories (85.5, 87.5, and 76.9
percent for traditional, modular, and unknown, respectively). The guard was not in use in 100 percent
of the cases where the operator did not receive a blade guard when the saw was acquired.
The blade guard was not in use in the majority of cases across each type of saw (87.0, 82.9, and 100.0
percent for bench, contractor/hybrid, and contractor saws respectively). There were 10 cases where the
type of saw was unknown, and the blade guard was not in use in any of these 10 cases.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

31
Table 21: Guard Use by Table Saw and Guard Characteristics in Table Saw Blade-Contact Injury Completed IDIs
n
Row %
Guard Use
Total
Yes
No
Unknown
N/A
Manufactured Guard Type
Traditional
9
8.8
91
89.2
1
1.0
1
1.0
102
Modular
3
12.0
22
88.0
0
0.0
0
0.0
25
Unknown
2
6.1
27
81.8
4
12.1
0
0.0
33
None
0
0.0
1
100.0
0
0.0
0
0.0
1
Total
14
141
5
1
161
Received with Saw Guard Type
Traditional
9
11.8
65
85.5
1
1.3
1
1.3
76
Modular
3
12.5
21
87.5
0
0.0
0
0.0
24
Unknown
2
7.7
20
76.9
4
15.4
0
0.0
26
N/A-None
0
0.0
35
100.0
0
0.0
0
0.0
35
Total
14
141
5
1
161
Table Saw Type
Bench
10
10.0
87
87.0
3
3.0
0
0.0
100
Contractor/Hybrid
4
9.8
34
82.9
2
4.9
1
2.4
41
Cabinet
0
0.0
10
100.0
0
0.0
0
0.0
10
Unknown
0
0.0
10
100.0
0
0.0
0
0.0
10
Total 14 141 5 1 161
SME Reviewed Diagnosis
Laceration
8
9.3
77
89.5
1
1.2
0
0.0
86
Severe Laceration
4
13.8
25
86.2
0
0.0
0
0.0
29
Amputation
2
8.3
20
83.3
1
4.2
1
4.2
24
Fracture
0
0.0
14
93.3
1
6.7
0
0.0
15
Avulsion
0
0.0
5
71.4
2
28.6
0
0.0
7
Total 14 141 5 1 161
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

32
Table 22 provides the cross-tabulated distributions for the type of guard manufactured with the saw by
when the guard was removed. For the 141 cases where the blade guard was not in use, the
distributions for when the blade guard was removed differ somewhat for the different type of blade
guards. The blade guard was removed after the saw was acquired in about 40 percent of the cases for
both traditional and modular blade guards. For the traditional blade guards, 22.0 percent were
removed before the saw was acquired while for modular blade guards, removal was at 4.6 percent.
Modular blade guards had a larger proportion that were never installed by the operator (36.4 percent
versus 13.2 for traditional blade guards).
Table 22: Guard Manufactured with Saw by When the Guard Was Removed in Table Saw Blade-Contact Injury
Completed IDIs Where the Blade Guard Was Not in Use (n = 141)
n
Row %
When was the guard removed?
(for guard in use = no)
Total
Guard Type
Manufactured with Saw
Prior to the
operator
acquiring
the saw
28
Never
installed
by
operator
After the
operator
acquired
the saw
Up position,
not removed
entirely
Unknown
Traditional
20
22.0
12
13.2
38
41.8
5
5.5
16
17.6
91
Modular
1
4.6
8
36.4
9
40.9
2
9.1
2
9.1
22
None
1
100.0
0
0.0
0
0.0
0
0.0
0
0.0
1
Unknown
13
48.2
3
11.1
3
11.1
1
3.7
7
25.9
27
Total
35 23 50 8 25 141
28
i.e., the operator did not receive a blade guard with the saw.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

33
The blade guard cannot be used in some types of cuts, such as when making a non-through cut. This is
not necessarily the reason the blade guard was or was not in use; see Table 20 for more information
about the reasons for blade guard removal. In Table 23, for the 141 blade-contact cases where the
blade guard was not in use, the guard type is cross-tabulated with the classification of through or non-
through cuts. Of the 22 cases with a table saw known to be manufactured with a modular blade guard,
4 cases (18.2 percent) involved a non-through cut. For the 91 cases known to be associated with a saw
manufactured with a traditional blade guard, but no blade guard was in use at the time of the incident, 7
cases (7.7 percent) involved a non-through cut.
Table 23: Guard Manufactured with Saw by Through/Non-through Cuts in Table Saw Blade-Contact Injury
Completed IDIs Where the Blade Guard Was Not in Use (n = 141)
n
Row %
Through Versus Non-Through Cuts
(for guard in use = no)
Total
Guard Type
Manufactured with Saw
Through
Non-Through
Other
Unknown
N/A
29
Traditional
71
78.0
7
7.7
1
1.1
11
12.1
1
1.1
91
Modular
14
63.6
4
18.2
0
0.0
4
18.2
0
0.0
22
Unknown
19
70.4
2
7.4
0
0.0
5
18.5
1
3.7
27
None
1
100.0
0
0.0
0
0.0
0
0.0
0
0.0
1
Total
105 13 1 20 2 141
29
“N/A” indicates that a cut was not being performed at the time of the incident. For example, one incident
occurred while the operator was cleaning saw dust from under the table top.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

34
Table 20shows that for 14 blade-contact injuries the blade guard was in use at the time of the injury,
and 141 blade-contact injuries occurred without a blade guard in use (while 5 were unknown if a blade
guard was in use and 1 where blade guard use was not applicable to the incident). Figure 1 summarizes
the usage of other safety devices that are part of the blade guard system, for cases with known blade
guard use. For the 141 without the blade guard in use, the majority were not using any other safety
devices as part of the system (53.2 percent), and 36.2 percent were unknown if any other device was in
use.
Figure 1: Saw Safety Devices by Blade Guard in Table Saw Blade-Contact Completed IDIs, when Blade Guard Use
is Applicable and Known (n=155 of the 161 cases)
n=141
n=14
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

35
Figure 2 shows the distribution for the operator personal protective equipment (PPE) in use at the time
of the incident. For the 161 table saw blade-contact injury completed IDIs, the operator wore
eyeglasses or safety goggles or safety glasses in 45 percent of the incidents. Eyeglasses were the most
commonly reported item (26 percent), and safety goggles or glasses were reported in 19 percent of the
cases (see Appendix C for details on how PPE information was collected). In 11 percent of incidents, the
operator was wearing or using multiple items. In 28 percent of incidents, the operator was reported to
not be using any additional PPE. Other types of PPE apart from safety glasses and eyeglasses, include,
for example, gloves and hearing protection.
Eyeglasses
26%
Mulitple
11%
None
28%
Other
3%
Safety glasses/goggles
19%
Unknown
13%
CT
Eyeglasses Mulitple None Other Safety glasses/goggles Unknown
Operator Safety Clothing/Gear (n=161)
Figure 2: Operator Personal Protective Equipment in Table Saw Blade-Contact Injury Completed IDIs
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

36
Table 24 shows the distributions of the alignment device use, how the stock was being pushed, the type
of cut, and the type of stock. Of the 161 table saw blade-contact injury completed IDIs, 84 (52.2
percent) reported to be using a rip fence, while 40 (24.8 percent) reported not to be using any
alignment device. There were 27 (16.8 percent) of the incidents with unknown alignment device use.
The majority of incidents involved the operator using their hand(s) to push (and in some cases, pull) the
stock through the cut, while 32 (19.9 percent) used a push stick or push block to push the stock through
the cut. The most common cut performed in the 161 incidents was a through/rip cut (102 cases, 63.4
percent), and wood was the identified stock type in 143 (88.8 percent) of the 161 cases.
Table 24: Incident Characteristics in Table Saw Blade-Contact Injury Completed IDIs
Variable
Frequency
Percent of Total
Total
161
100%
Alignment Device in Use
None (free hand)
40
24.8
Rip fence
84
52.2
Miter gauge
1
0.6
Other
7
4.4
Unknown
27
16.8
N/A
2
1.2
How was the stock being
pushed through the blade?
Hand(s)
102
63.4
Push stick
31
19.3
Push block
1
0.6
Other
6
3.7
Unknown
18
11.2
N/A
3
1.9
Type of Cut
Through/rip
102
63.4
Through/cross
12
7.5
Through/other
6
3.7
Non-through/rip
12
7.5
Non-through/other
3
1.9
Other
1
0.6
Unknown/rip
6
3.7
Unknown
16
9.9
N/A
3
1.9
Stock Type
Wood
143
88.8
Other
11
6.8
Unknown
4
2.5
N/A
3
1.9
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

37
Table 25 provides summary statistics for the reported dimensions of the stock being cut in table saw
blade-contact injury completed IDIs. The SME review team coded the dimensions in descending order
for length, width, and thickness of the recorded dimensions, not in relation to the type of cut being
made. In other words, the length is always the longest dimension in each case. Thus, this gives a sense
to the size of the stock in these injury cases, but not how these dimensions relate to the cut that was
being performed. The number of missing cases is 41, 35, and 36 for length, width, and thickness,
respectively, in the 161 cases.
Table 25: Stock Dimensions in Table Saw Blade-Contact Injury Completed IDIs
Stock
Dimension
n
n missing
minimum
25
th
percentile
median
75
th
percentile
maximum
Length
120
41
3.00
12.0
24.0
48.0
144.00
Width
126
35
0.25
2.00
4.00
5.50
36.00
Thickness 125 36 0.13 0.50 0.75 1.33 4.00
Table 26 summarizes in a general manner classification how blade contact occurred in the 161 cases of
table saw blade-contact completed IDIs, and then provides the additional details the SMEs coded for the
cases where the victim’s hand was not pulled into the blade. In the majority of cases, 56.6 percent,
blade contact did not involve the victim’s hand being pulled into the blade (91 cases). In 45 of the 161
cases (28.0 percent), blade contact occurred by the victim’s hand being pulled into the blade during the
incident, and in 24 cases (14.9 percent) how the victim’s hand made contact with the blade could not be
determined. Among the 91 cases where the victim’s hand was not pulled into the blade, the SME
review team determined that the victim was reaching to do, or for, something in 46.2 percent of the
cases, and the victim’s hand was fed into the blade in 17.6 percent of the cases. The remaining cases for
the victim’s hand not pulled into the blade, and for which details were available to further classify the
blade contact, included situations where the victim inadvertently moved his/her hand into the blade,
the hand slipped or dropped off the workpiece, or some other scenario.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

38
Table 26: How Blade Contact Occurred in Table Saw Blade-Contact Injury Completed IDIs
Variable
Frequency
Percent of Total
How did blade contact occur?
(High-level categories)
Hand not pulled into blade
91
56.5
Hand pulled into blade
30
45
28.0
Other
1
0.6
Unknown
24
14.9
Total
161
100%
Hand not pulled into blade (additional details)
Hand fed into blade (with workpiece)
16
17.6
Hand slipped or dropped off workpiece
7
7.7
Inadvertently moved hand into blade 12 13.2
Hand reached
42
46.2
Other
5
5.5
Additional details unknown
9
9.9
Total
91
100%
Table 27 provides the breakdown of blade-contact, completed IDI cases by type of guard manufactured
with the saw by how blade contact occurred (using the high-level categories), regardless of whether the
guard was in use at the time of the incident. For saws manufactured with a traditional blade guard, in
55.9 percent of the cases, the victim’s hand was not pulled into the blade, while in 32.4 percent of the
cases, the victim’s hand was pulled into the blade. Saws manufactured with a modular blade guard had a
similar breakdown into how blade contact occurred (56.0 percent of cases the victim’s hand was not
pulled into the blade and 28.0 percent of the cases, the hand was pulled into the blade). As previously
noted, there is a small number of cases for modular blade guard saws, in general, so caution should be
used in drawing conclusion by taking this into account.
Table 27: Manufactured Guard Type Versus How Blade Contact Occurred (High-Level Categories) in Table Saw
Blade-Contact Injury Completed IDIs
n
Row %
How did blade contact occur?
(High-level categories)
Total
Guard Type
Manufactured with Saw
Hand not pulled
into blade
Hand pulled
into blade
Other
Unknown
Traditional
57
55.9
33
32.4
1
1.0
11
10.8
102
Modular
14
56.0
7
28.0
0
0.0
4
16.0
25
None
0
0.0
0
0.0
0
0.0
1
100.0
1
Unknown
20
60.6
5
15.2
0
0.0
8
24.2
33
Total
91
56.5
45
28.0
1
0.6
24
14.9
161
30
One case involved the victim’s arm being pulled into the blade. This case is in the “hand pulled into blade”
category because it fits the general pattern of being pulled, with the only distinguishing feature being that an arm
was pulled instead of a hand. The “circumstance” variable captures the unique aspect of this case.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

39
Table 28 provides the breakdown of the 161 table saw blade-contact injuries by whether unexpected
workpiece movement occurred prior to blade contact. Unexpected workpiece movement includes, but
is not limited to, kickback. Unexpected workpiece movement did not occur in 47.8 percent of the
incidents, did occur in 39.8 percent, and was unknown in 10.6 percent of the incidents.
Table 28: Unexpected Workpiece Movement in Table Saw Blade-Contact Injury Completed IDIs
Unexpected Stock Movement
Frequency
Percent of Total
Yes
64
39.8
No
77
47.8
Unknown
17
10.6
N/A
3
1.9
Total 161 100%
Table 29 provides the cross-tabulation of type of guard manufactured with the table saw versus whether
unexpected workpiece movement occurred during the incident, for all blade-contact completed IDIs,
regardless of whether the guard was in use or not at the time of the incident. For traditional blade
guards, unexpected workpiece movement was reported to have occurred in the same number of cases
as when unexpected workpiece movement was not reported to have occurred (45.1 percent for
traditional blade guard saws); for modular blade guard saws, unexpected workpiece movement was
reported in 9 cases and in 13 cases (36.0 percent and 52.0 percent of modular blade guard saws
respectively).
Table 29: Manufactured Guard Type Versus Unexpected Workpiece Movement in Table Saw Blade-Contact
Injury Completed IDIs
n
Row %
Unexpected Stock Movement
Total
Guard Type
Manufactured with Saw
Yes
No
Unknown
N/A
Traditional
46
45.1
46
45.1
8
7.8
2
2.0
102
Modular
9
36.0
13
52.0
3
12.0
1
3.0
25
None
0
0.0
0
0.0
1
100
0
0.0
1
Unknown
9
27.3
18
54.6
5
15.2
1
3.0
33
Total
64
39.8
77
47.8
17
10.6
3
1.9
161
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

40
To further understand how blade contact occurred, the unexpected workpiece movement variable is
evaluated in additional detail in Tables 30, 31, and 32, and in Figure 3.
Table 30 considers how blade contact occurred in general with whether there was unexpected
workpiece movement during the incident. For incidents where the hand was not pulled into the blade,
the majority of incidents (75.8 percent) did not involve unexpected workpiece movement; in incidents
where the hand was pulled into the blade, the majority of incidents involved unexpected workpiece
movement.
Table 30: How Blade Contact Occurred Versus Unexpected Workpiece Movement
in Table Saw Blade-Contact Injury Completed IDIs
n
Row %
Unexpected Workpiece Movement
Total
How did blade contact occur?
(High-level categories)
Yes
No
Unknown
N/A
Hand not pulled into blade
15
16.5
69
75.8
4
4.4
3
3.3
91
Hand pulled into blade
41
91.1
3
6.7
1
2.2
0
0.0
45
Other
0
0.0
1
100.0
0
0.0
0
0.0
1
Unknown
8
33.3
4
16.7
12
50.0
0
0.0
24
Total
64
77
17
3
161
Table 31 provides how blade contact occurred with the use of a blade guard. Only 14 of the 161
incidents occurred with the blade guard in use, so any comparisons are quite limited here. However,
note that the proportion of cases in which the blade guard was not in use is similar for both the hand
pulled and not pulled into the blade categories.
Table 31: How Blade Contact Occurred Versus Blade Guard Use in Table Saw Blade-Contact Injury Completed
IDIs
n
Row %
Blade Guard Use
Total
How did blade contact occur?
Yes
No
Unknown
N/A
Hand not pulled into blade
6
6.6
80
87.9
4
4.4
1
1.1
91
Hand pulled into blade
5
11.1
39
86.7
1
2.2
0
0.0
45
Other
0
0.0
1
100.0
0
0.0
0
0.0
1
Unknown
3
12.5
21
87.5
0
0.0
0
0.0
24
Total 14 141 5 1 161
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

41
Figure 3 and Table 32 provide similar information, with the circumstance that the SME review team
determined to correspond to how blade contact occurred. For the hand being pulled into the blade, the
SME review team determined unexpected workpiece movement to be the most significant event or
cause leading to blade contact; in incidents where the hand was not pulled into the blade, removing the
workpiece or cutoff, or some other action, are the most common significant event or cause leading to
the blade contact. This does not mean that unexpected workpiece movement did or did not occur in
any given case; there is another variable capturing the event of unexpected workpiece movement (see
Table 28). As seen in Table 32, different circumstances stand out for different categories of the hand
not being pulled into the blade.
Figure 3: Circumstance for How Blade Contact Occurred in Table Saw Blade-Contact Injury Completed IDIs
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

42
Table 32: Circumstances Leading to Blade Contact in Table Saw Blade-Contact Injury Completed IDIs
How did blade contact occur?
Circumstances Leading to Blade
Contact
Frequency
Percent of
Blade Contact
Category
Percent of
Total (n=161)
Hand not pulled into blade/
hand fed into blade (with workpiece)
Adjusting workpiece position
2
12.5
1.2
Distracted
1
6.3
0.6
Nothing unusual/cutting workpiece
10
62.5
6.2
Other
3
18.8
1.9
Total
16
100%
9.9%
Hand not pulled into blade/
hand reached
Adjusting workpiece position
2
4.8
1.2
Dislodging jam
2
4.8
1.2
Other
9
21.4
5.6
Reaching around/over blade
5
11.9
3.1
Removing cutoff/workpiece
23
54.8
14.3
Unknown
1
2.4
0.6
Total
42
100%
26.1%
Hand not pulled into blade/
hand slipped or dropped off workpiece
Distracted
1
14.3
0.6
Other
2
28.6
1.2
Switching off saw (blade slowing)
4
57.1
2.5
Total
7
100%
4.3%
Hand not pulled into blade/
inadvertently moved hand into blade
Distracted
1
8.3
0.6
Other
7
58.3
4.4
Removing cutoff/workpiece
1
8.3
0.6
Switched off saw (blade slowing)
3
25.0
1.9
Total
12
100%
7.5%
Hand not pulled into blade/
other
Removing cutoff/workpiece
3
60.0
1.9
Other
2
40.0
1.2
Total
5
100%
3.1%
Hand not pulled into blade/
additional details unknown
Other
1
11.1
0.6
Unknown
8
88.9
5.0
Total
9
100%
5.6%
Hand pulled into blade
Removing cutoff/workpiece
2
4.4
1.2
Unexpected workpiece movement
36
80.0
22.4
Other
6
13.3
3.7
Unknown
1
2.2
0.6
Total
45
100%
28.0%
Other
Other
1
100 0.6
Total
1
100%
0.6%
Unknown
Nothing unusual/cutting workpiece
1
4.2
0.6
Unexpected workpiece movement
7
29.2
4.4
Other
1
4.2
0.6
Unknown
15
62.5
9.3
Total
24
100%
14.9%
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

43
X.
Appendix A: Estimation Methodology for a Field Staff Investigation Study of
the NEISS
The 2017 Study is the first study of its type that CPSC has undertaken. CPSC staff designed the study to
address an inability to identify specific table saw type in injury data, among other data collection goals
(see the “Introduction” section for study goals).
31,32
The study’s design uses the statistical structure of
the NEISS, while incorporating non-survey-based CPSC Field staff investigations for follow-up data
collection, which potentially opens multiple sources of variation that cannot be measured individually,
and therefore, cannot be accounted for directly in the variance calculations.
Staff reviewed each NEISS case in the timeframe set for product codes 0841 (table saws), 0845 (saws,
not specified), and 0895 (power saws, other or not specified). A case was assigned for investigation
follow-up, if staff determined that the injury could have been a table saw blade-contact injury, or if
unknown as table saw blade-contact injury. Thus, the methodology to analyze the results needed to
leverage the complex survey structure of the NEISS, incorporating the structure that most cases were
assigned, but not all cases (thus, information for the questions at hand come from multiple stages of the
study, see Appendix B for the flow chart of data collection and connection to estimation methodology),
and incorporating the Field investigation-based data collection. No investigation was requested on the
cases where the information in the NEISS case indicated that there was no blade contact or no table saw
involved, due to the increase in resources required for a Field investigation-based study. In a CATI-based
survey, all cases would be assigned for further data collection, due to the minimal costs and
simplification of the methodology needed. However, the cases not assigned for investigation, because it
is known from the NEISS narrative to have not involved either a table saw or blade contact, remain vital
to the analysis process, because the goal is to estimate adjustment factors that can be employed across
multiple years of the NEISS, not to generate an estimate for one year. This also means that CPSC’s
typical survey methods cannot be used for analyzing the study’s entirety. Therefore, CPSC staff
developed a new methodology specifically to analyze this type of study, using statistical methods for
surveys (incorporating the complex survey structure of the NEISS structure) and investigation-based
data collections.
The following summarizes the methodology developed by staff to analyze a CPSC Field data collection of
a NEISS-based study. The methodology description here incorporates the language of the 2017 Study;
however, as noted above, the generalized methodology can be applied to any study similarly designed.
All resulting 95 percent confidence intervals are obtained assuming a normal distribution.
31
Garland, Sarah. “Addendum to ‘Survey of Injuries Involving Stationary Saws: Table and Bench Saws, 2007−2008:
Evaluation of Response Integrity and Resulting Estimates for Types of Saws and Types of Drives’” Memorandum to
Caroleene Paul, April 14, 2014. Consumer Product Safety Commission.
http://www.cpsc.gov//Global/Research-
and-Statistics/Injury-
Statistics/Home%20Maintenance%20and%20Construction/CoverpageandMemoofStaffAnalysisofTableSawTypeinN
EISSSpecialStudy.pdf
32
Stralka, Kathleen. “2014-2015 Table Saw Special Study Cautionary Statement” Memorandum to Caroleene Paul,
November 21, 2016. Consumer Product Safety Commission, Table Saw NPR Briefing Package, Tab F.
https://www.cpsc.gov/s3fs-public/Proposed%20Rule%20-%20Safety%20Standard%20for%20Blade-
Contact%20Injuries%20on%20Table%20Saws%20-%20January%2017%202017.pdf
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

44
Statistical Estimation Methodology Using CPSC’s Field Investigations Follow-Ups for
NEISS Cases
Notations
Number of hospitals in stratum
Number of cases in hospital in stratum
Number of bootstrap samples
Weight for case in hospital in stratum ; adjusted weights donated by prime and double
prime depending on the stage adjustment is made (
and
)
Bootstrap estimate of the proportion for Level-1 questions
33
Bootstrap estimate of the proportion for Level-2 questions
34
NEISS injury estimate
Injury estimate for Level-1 questions
Injury estimate for Level-2 questions
Set of hospitals in stratum
()
Set of hospitals for bootstrap sample in stratum
Indicator variable for case in hospital in stratum
(
)
Proportion for bootstrap sample in stratum
Mean of the proportion within stratum for all bootstrap samples
(
)
Proportion for bootstrap sample
Bootstrap estimate of the proportion
33
Level 1 questions are evaluated using the NEISS case information when a case was not assigned for investigation
as a “no” in the yes/no response of the question, and the “yes” and “unknown” are assigned for follow-up
investigations. Thus, data to answer the question come from two stages in the study, either from the NEISS case,
or the completed investigation. For example, was the injury related to blade contact on a table saw?
34
Level 2 questions can only be answered through the set of completed investigations, which is a subset of the
cases for the Level 1 questions. For example, what type of table saw was involved in the table saw blade-contact
injury?
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

45
(1) Adjust NEISS weights to account for non-participating NEISS hospitals
35
(i.e., NEISS hospitals that
do not provide victim contact information a priori).
The adjusted weight can be written as
=
w
here
=
1,
0,
a
nd
is the adjustment calculated based on post-stratification/raking. This has been simplified for
reading ease here; exactly how hospital/unit nonresponse is handled is developed based on the specifics
of a given study. For the 2017 Study, post-stratification was applied to rake to each stratum’s marginal
totals.
can be written as
=
,
0
,
.
T
hus, subsequent steps only use the set of cases with a non-zero
.
(2) Determine datasets to use for estimation process and rake/post-stratify for Level 1 and Level 2
estimates (See Appendix B for a flow chart of information collection for Level 1 and Level 2
estimates).
For each level estimate, incorporating the information that comes from both NEISS case records and
completed IDIs, proportionally allocate (i.e., post-stratify or rake) “No ID Received” cases and
“Terminated” cases (nonresponse) to the set of cases of the most appropriate completed set, depending
on the study details and estimate levels. For the cases that a request for investigation was submitted,
investigation-unit nonresponse for the 2017 Study, post-stratification/raking was applied using the
variables stratum, age group, product code (0841 versus not), and diagnosis from the NEISS, as these
variables showed a difference in response propensities for all strata except children’s stratum. The
children’s stratum only had 2 completed IDIs; thus, the children’s strata was raked to the marginal total
for the stratum without any other variables.
See Appendix B for additional details of the information collection stages for this analysis process.
35
A “participating hospital” is defined as an active NEISS hospital that provides patient identification, if available,
on a case-by-case basis, as requested by CPSC staff. A “non-participating hospital” is an active NEISS hospital that
never provides any patient identification to CPSC as part of their contract.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

46
L
et
=
wh
ere
is the original weight all cases in product codes 0841, 0845, 0895.
Let
be the estimated proportion of that are positive to be a table saw blade-contact injury.
is
independent of .
Let
be the estimated number of table saw blade-contact, injuries, as
=
and
=
+
(
)
+
(
)
(
).
Q
uestions that can only be answered through a completed investigation (e.g., type of table saw and
blade guard use) are Level-2 estimates, but are based on a subset of Level-1 data/estimates. Let
be
the proportion of
that is positive for the Level-2 question.
Thus,
=
and
=
.
is independent of
;
36
however,
and
are dependent. Therefore,
=
(
)
+
+
(
)
(
)
a
nd
=
=
,
+
+ (
)
+ (
)
,
+
.
All
and
are bootstrap estimates.
37
The same methodology is used to obtain each bootstrap
estimate, so the notation of
will be used through the bootstrap methodology, whenever the
methodology is interchangeable for
and
.
36
Independence does not mean the covariance must be zero. However, until otherwise known (testing can be
completed by the analyst, as needed), the assumption is that the covariance between and
is zero.
37
Bootstrapping is a resampling with replacement technique that allows for an estimated distribution to be
generated for a sample estimate, when the distribution cannot be assumed or calculated. Using the law of large
numbers, inferences can then be made for the measure of interest.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

47
and
estimates calculated from this study can be applied, with their associated variance
estimates, to other NEISS years in the same manner as above, as deemed appropriate. The following
steps provide the estimation methodology to obtain
and
.
(3) Obtain estimates
and
via bootstrapping at the PSU (hospital) level.
Bootstrapping requires an independent and identical distribution. The NEISS hospitals are the primary
sampling units (PSUs) in the NEISS, and also where the independent and identical distributions occur
(only within stratum, not across strata). Independent and identical distributions do not occur at the
individual case level, regardless of whether there is an investigation or not for the case.
38
Thus, when
bootstrapping the NEISS, the hospitals (PSUs) are selected as the variable to bootstrap, then all cases
from each PSU selected are included in the bootstrap sample to form the whole sample.
L
et
=
{
|= 1, … ,
}
be the set of PSUs within stratum where = 1, … ,5 and
is the number of
PSUs within stratum .
Let
()
=
()
|
()
= 1, … ,
be the
bootstrap sample of PSUs from
, where = 1, … , .
39
3.1 Generate a bootstrap sample,
(
)
, of size
from
, selecting with replacement. Select all
cases,
= 1, … ,
in each
()
selected to form the full bootstrap sample. For the first pass
through, = 1.
3.2 To accommodate the strata structure of the NEISS for variance component calculations steps in 3.4
and 3.7, calculate the proportion of “yes” for
()
, = 1, . . . , .
(
)
=
wh
ere
=
1,
0, .
3.3 Repeat steps 3.1 through 3.2 times.
3.4 To accommodate the strata structure in the NEISS for variance calculations in 3.7, calculate
=
1
()
.
3.5 Repeat steps 3.1 through 3.4 until each stratum is completed, = 1, . . . ,5.
38
Givens, Geof and Hoeting, Jennifer A. Computational Statistics. Hoboken, NJ: John Wiley & Sons, Inc., 2005.
39
For the 2017 Study, B=1000.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

48
3.6 Combine all bootstrap samples from
()
for = 1, … 5 for each , = 1, . . . , .
()
=
()
,
()
,
()
,
()
,
()
For = 1, … , , calculate
()
=
wh
ere
=
1,
0, .
3.7 Calculate the bootstrap estimates
=
1
()
=
1
1
(
)
,
=
1
1
(
)
(
)
.
Fo
r
,
, the above is simply adjusted accordingly to incorporate the square terms. The
notation gets too cluttered to read easily; however, the calculations follow easily from what is given.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

49
Table 29 provides the bootstrap bias estimates
40
for each of the bootstrap estimates obtained in the
2017 Study. Bootstrap bias estimates were small and did not affect the subsequent results of the study.
Table 33: Bootstrap Bias Estimates for Level 1 and Level 2 Theta Estimates
Bootstrap Estimate Identifier
Bootstrap Bias
Estimate for
Bootstrap Estimate Identifier
Bootstrap Bias
Estimate for
Table Saw Blade Contact (Level 1:
)
< 0.0001
Table Saw Type (Level 2:
)
Disposition (Level 2:
)
Bench
0.0007
Treated and Released
0.0008
Contractor
-0.0005
Hospitalized
-0.0006
Cabinet
-0.0004
Other
*
Unknown
*
Body Part (Level 2:
)
Blade Guard Use (Level 2:
)
Finger -0.0002
No
-0.0001
Hand
0.0001
Yes
0.0005
Sex (Level 2:
)
Unknown
-0.0002
Male
-0.0001
N/A
*
Female
0.0001
Guard Type Manufactured
with Saw (Level 2:
)
Age Group (Level 2:
)
Traditional
-0.0015
≤40
-0.0008
Modular
0.0003
41-60
0.0003
Unknown
0.0010
≥61
0.0005
N/A
*
Diagnosis (Level 2:
)
Laceration
0.0013
Fracture
-0.0006
Amputation
-0.0004
Other
-0.0003
Reviewed Diagnosis (Level 2:
)
Laceration
0.0010
Severe Laceration
0.0005
Amputation
-0.0006
Fracture or Avulsion
-0.0008
40
A bootstrap estimator is a bias estimator, and it is possible to understand the bias for the bootstrap estimator, in
particular in this study’s application of the bootstrap methodology. In a bootstrap estimate, the bias is the
difference between the original sample proportion and the average of all the bootstrap samples’ proportions for
the proportion of interest.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

50
XI.
Appendix B: NEISS Case Assignment Process Flow
Case has product code 0841, 0845, or 0895
No
End
Yes
Participating hospital?
No
End
Yes
Involved a table saw?
No
End
Yes/Unknown
Involved blade contact?
No
End
Yes/Unknown
Request Field investigation
Victim identification received from hospital?
No
End
Yes
Sent to Field staff for investigation
Contact made with victim and
cooperation gained
No
End
Yes
Involved a table saw?
Yes
Is blade contact?
Table saw type?
No
Collect information about product
and the incident
Other incident information
Level 2 Questions
Level 1 Questions
Note: At the investigation
level, a case previously
considered in-scope can
become out-of-scope (e.g., it
becomes known that the
saw was a homemade table
saw or the incident was
work related). While this
methodology
accommodates cases where
a completed investigation
indicates an out-of-scope
status, there are a small
number of cases that are not
assigned based on the NEISS
information, and the scope
is assumed. Thus, this small
proportion of unassigned
cases may include some
cases that would be
considered out-of-scope if
more information were
known. However, this
would only be expected for a
small number of the already
small proportion of
unassigned cases. Thus, this
does not have a significant
impact on estimates
obtained through this
methodology.
Level 1 Questions
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

51
XII.
Appendix C: SME IDI Review Process and Variable Descriptions
A team of CPSC SMEs reviewed each completed investigation in the 2017 special study. The team
consisted of a mechanical engineer, a physiologist, a human factors engineer, an economist, and a
statistician. This section describes the process for reviewing and coding completed IDIs from the 2017
Study and also describes the final set of variables coded by the review team and used for this report.
There were two types of completed investigations for the review team. One type is an investigation
where the product was a table saw and the other is where the product was not a table saw. If the
product was not a table saw, the review team ensured that there was consensus for the type of product
involved, and nothing further was assessed in these investigations, though they play a vital role in the
Appendix A methodology as part of the denominator for the Level 1 adjustment factor estimates and
also in any future calculations for different product injury estimate analyses.
For investigations where a table saw was identified, the review process became more involved. Each
SME independently reviewed all the available information for each case and coded each variable based
on their review. The sets of coding from the SMEs were compared for each case and differences in
coding identified. For any differences in coding, the SMEs discussed the details of the case and reached
a consensus on any differences. The final set of coding reflects SME agreement on each variable for
each case.
Also, the SMEs developed the list of variables and any categories within the variables. Not all categories
for all variables are reported in the results sections, due to the lack of use of some categories in coding
the incidents. The following are the descriptions of the variables used for completed investigations that
identified a table saw within the 2017 special study that are used within this report. There were
additional variables coded by the SMEs; however, they were not used directly or indirectly within this
report, but are available for further understanding of the scenarios surrounding these incidents; these
variables are free text in format and contain too wide a variety of input to categorize and subsequently
summarize in this report.
The format for each variable described in this section is as follows:
Label (variable name, as in the analytic dataset): Description. (Format: Description).
Categories listed.
NEISS Variables
The NEISS captures data for several variables used in the results of this report. However, based on the
additional information captured via an IDI, some cases required an adjustment to the recorded value of
a NEISS variable. For example, the “type” variable (was the injury occupational-related?) records a “not
work-related” or “unknown if work-related” value in the NEISS; however, upon interviewing the victim
through the IDI process, additional information reveals that the injury was work-related. Therefore, the
case should be considered as out-of-scope for the purposes of this report. Because the case still “lives”
in the NEISS, and thus in any estimates that include it, it is not deleted from this analysis, but used to
inform the analyses. Thus, this corrected value for “type” is captured in the “type_correction” variable
in the analytic dataset for this report. This report relies on the corrected values, not the original NEISS
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

52
coding. This section describes the NEISS variables used and the corresponding correction variables, if
applicable.
For information on the values these variables can take and variable types related to these variables, the
NEISS coding manual is available at CPSC.gov.
41
These variables are considered auxiliary variables in this
analysis, because they are available for all cases, whether a follow-up investigation was completed or
not. However, only completed IDIs can inform any correction variables’ values.
Age Group (age_group): The NEISS records age, not age group; however, for the purposes of this
analysis, staff grouped ages as: ≤40, 41-60, and ≥61. (Format: Categorical)
Sex (sex): The NEISS variable that records the victim’s sex. (Format: Categorical)
Body Part (bdpt): The body part as recorded in the NEISS. SME corrections to the body part involved
are found in the body part correction variable in the analytic dataset for this report (bdpt_correction).
(Format: Categorical)
Diagnosis (diag): The diagnosis as recorded in the NEISS. SME corrections to the NEISS diagnosis are
found in the diagnosis correction variable in the analytic dataset for this report (diag_correction).
(Format: Categorical)
Disposition (disp): The disposition as recorded in the NEISS. (Format: Categorical)
Occupational Injury (type): The occupational injury (type) identifier as recorded in the NEISS. SME
corrections to the NEISS type are found in the type correction variable in the analytic dataset for this
report (type_correction). (Format: Categorical)
Saw Variables
Product Involved (isTableSaw): This variable is only reported in Table 5 for all cases with completed IDIs,
as part of the completed IDI tracking, and this variable is part of this tracking. Only the set of completed
table-saw IDIs are in the analytic dataset, so “isTableSaw” has the values of “yes.” However, this
variable, as part of the completed IDI tracking process, is used throughout the report for calculations.
(Format: Categorical). Table 5 contains the categories of this variable.
Homemade table saw identifier (scope): While the NEISS captures homemade table saws in the table
saw product code (0841), though a rare event, for the purposes of rulemaking efforts, homemade saws
are not in the scope of interest, and are excluded from the table saw blade-contact injury set. The
results of this variable are not listed in this report, but the results are used in calculations throughout.
(Format: Indicator)
Values:
1 = yes, homemade (not manufactured table saw)
. = missing values indicate a manufactured (in-scope) table saw
41
https://cpsc.gov/neiss/completemanual.pdf
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

53
Table Saw Type (TableSawType): Captures the SME determination of the type of table saw involved in
the incident. (Format: Categorical)
Categories:
Bench or jobsite saw
Contractor saw
42
Cabinet saw
Hybrid saw
Other
Unknown
Guard Type Manufactured with Saw (guard_mfr): The SME determination of the type of blade guard the
incident table saw was manufactured with, regardless to the guard’s availability for use at the time of
the incident and the circumstances of the incident. (Format: Categorical)
Categories:
Traditional
Modular
Other
Unknown
Guard Type Received by Operator when Saw Acquired (guard_received): Identifies the type of blade
guard the user/owner received when s/he acquired the saw (e.g., when the saw was bought (used or
new), borrowed, rented, etc.). (Format: Categorical)
Categories:
Traditional
Modular
Other
N/A-None received (when the operator acquired the saw)
Unknown
Use frequency of the incident saw (use_freq): This variable records the operator’s use frequency of the
incident table saw. (Format: Categorical). If additional information beyond these categories was
provided, the information falls into these categories but was described differently than these categories,
or if the use frequency description fit into the “other” category, the additional information is recorded in
the “other_use_freq” variable.
Categories:
First time
Daily to weekly
Weekly to monthly
Monthly to yearly
Yearly
Other
Unknown
42
The “contractor saw” and “hybrid saw” categories were collapsed for analysis purposes.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

54
Injury Variables
Was the injury related to blade contact? (blade_contact): Captures if the injury was caused by the
victim making contact with the table saw blade. (Format: Categorical)
Categories:
Yes
No
Unknown
Was the operator the injured person? (operator_inj): Indicates if the operator was the injured party,
and if not the operator, who was injured. (Format: Categorical). If the category is “No,” then the
“not_op_who” variable provides information about who was injured.
Categories:
Yes
43
No (identified in the “not_op_who” variable)
Unknown
Injury Description (injury_dscrp): SME description of the injury (injuries). See (Goldsmith, 2018) for the
discussion regarding injuries associated with table saw blade contact. (Format: Free text)
SME injury diagnosis (reviewed_diag): The SME determination for the diagnosis. This variable is
described further in the text in Section VII and IX with results compared to the NEISS diagnosis. (Format:
Categorical)
Injured hand (injured_hand): Identification of the injured hand. (Format: Categorical)
Categories:
Left
Right
Both
Unknown
Dominant hand (dominant_hand): Identification of the victim’s dominant hand. (Format: Categorical)
Categories:
Left
Right
Both (i.e., ambidextrous)
Unknown
43
Operators are not necessarily the owners or person responsible for the saw’s overall maintenance, but is the
person responsible for the operation of the saw at the time of the incident.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

55
Incident Variables
Blade Guard Use (guard_use): Indicates if the blade guard was in use (i.e., attached and in the down
position) at the time of the incident. (Format: Categorical)
Yes
No
N/A
44
Unknown
When the guard not in use, why was it not in use and when was it removed? (why_noGuard_categories
and when_guard_removed): These two variables were created after all coding was completed, based
on the information SME coded in the variable “why_noGuard,” which is a free text variable where SME
recorded all the information available for why a blade guard was not in use. The “why_noGuard”
variable contains more details that inform these two variables. This free text variable was reviewed
after the IDI review process was completed, and these two variables and their categories were created,
based on the patterns discovered. (Format: Categorical)
When was the guard removed?
(when_guard_removed)
Categories:
Why was the guard removed?
(why_guard_removed)
Categories:
Prior to [the saw’s] acquisition
45
Never installed
After [the saw’s] acquisition
[Guard in the] up position, not removed entirely
Unknown
Did not receive a guard when saw acquired
Inconvenient/visibility/cut type/stock size
Broken
Lost
Difficulty installing
Other
Combination of these (each listed)
Unknown
44
Some variables have the category of “N/A” as an option. The “N/A” category is limited to situations where the
variable cannot apply, like a person tripping over a saw that was not in use or cleaning underneath the table saw
table top and accidently turning the saw on. Even if a person is not actively cutting a piece of stock (e.g., is
between cuts, just finished a cut, or is retrieving a new piece of stock to cut), the existence of a safety feature, for
example, is important to note. For an incident occurring in-between cuts, almost all variables are considered
applicable, including unexpected stock movement, alignment devices, safety devices, stock type, etc., and so all are
coded without using the “N/A,” regardless of how the consumer or investigator answers in the IDI.
45
i.e., the operator did not receive a blade guard with the saw
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

56
How did the blade contact occur? (how_blade_contact): SME determination of the cause of blade
contact (an attached, intact blade), whether the hand was pulled or not pulled into the blade, and
additional information as available for the hand not being pulled into the blade. (Format: Categorical) If
an “other” category is chosen, additional information is in the “other_how_BC” variable.
Categories:
Hand not pulled into blade/hand fed into blade (with workpiece)
Hand not pulled into blade/hand reached
Hand not pulled into blade/hand slipped or dropped off workpiece
Hand not pulled into blade/inadvertently moved hand into blade
46
Hand not pulled into blade/other (specified in the “other_how_bc” variable)
Hand not pulled into blade/additional details unknown
Hand pulled into blade
Other (specified in the “other_how_bc” variable)
No blade contact/not kickback-related
47
No blade contact/workpiece kickback with victim struck
No blade contact/other
46
The victim is not intentionally reaching for something or to do something.
47
The “blade_contact” variable, described earlier, contains the information about the injury being related to blade
contact or not. The information is repeated here for incidents without blade contact to help any analyst recall the
scope of the study accurately. No conclusions can be drawn for no-blade-contact incidents, because only blade
contact or unknown blade contact incidents were assigned for follow-up investigation, with the goal to obtain
information only for blade-contact injuries. These cases are the no-blade-contact cases within assigned and
completed cases only, not the whole set of table saw injuries that are not related to blade contact. These
categories are not reported in Sections VII or IIX, because they do not apply to the blade-contact set of injuries.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

57
Circumstances leading to or at blade contact (circumstance): SME determinations answering: What
happened immediately before blade contact (preceding action of “how did blade contact occur?”), or
what is the most important circumstance before/at blade contact? This variable provides additional
details for circumstances to the “How did blade contact occur?” variable; thus may sometimes be
redundant information to “how did blade contact occur?”
Also, it is not necessary that an incident with
unexpected stock movement have the immediate or most significant circumstance to blade contact be
the unexpected workpiece movement, though it certainly can be. (Format: Categorical). When an
“other” category is chosen, additional information is in the “other_circum” variable.
Categories:
Adjusting workpiece position
Dislodging jam
Distracted
Nothing unusual/cutting workpiece
Reaching around/over blade
48
Removing cutoff/workpiece
49
Switched off saw (blade slowing)
Unexpected workpiece movement
Other (specified in the “other_circum” variable)
No blade contact/other (specified in the “other_circum” variable)
No blade contact/unexpected workpiece movement
Unknown
Unexpected stock movement (unexp_stock_move): Indicates if the stock moved in an unexpected way
(this includes, but is not limited to, stock kickback), regardless of determination, if this lead to the blade
contact. (Format: Categorical)
Categories:
Yes
No
N/A
Unknown
Alignment device in use (align_device): Identifies the type of alignment device in use, if any, at the time
of the incident. (Format: Categorical). When an “other” category is chosen, additional information is in
the “other_align_device” variable.
Categories:
Rip fence
Miter gauge
Sled
Jig
Other (specified in the “other_align_device” variable)
None (free hand)
N/A
Unknown
48
Reaching around/over blade: The person was reaching around or over the blade for some reason other than
removing a cutoff or the workpiece.
49
Removing cutoff/workpiece: The person was attempting to remove the cutoff or workpiece. It doesn’t matter
whether contact with the blade was during the reach or during the retraction.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

58
How was the stock being pushed through the blade? (how_pushed) Identifies how the victim was
pushing the stock during the cut. (Format: Categorical). When an “other” category is chosen, additional
information is in the “other_pushed” variable.
Categories:
Hand(s)
Miter Gauge
Push block
Push stick
Sled
Other (specified in the “other_pushed” variable)
N/A
Unknown
Saw safety devices (saw_safety_all): Excluding the blade guard (see blade guard questions), this
provides the use of other the safety devices with table saw guard assembly, not what the operator was
wearing, at the time of the incident. This variable summarizes the detailed information available in the
variable “saw_safety1, “saw_safety2,” and “other_saw_safety.” (Format: Categorical)
Categories:
None
Riving knife
Spreader
50
Anti-kickback pawls
Riving knife + Anti-kickback pawls
Spreader + Anti-kickback pawls
Other + Anti-kickback pawls
N/A
Unknown
Stock type (stock_type): This describes the type of stock being cut in a general category (e.g., wood
laminate flooring is in the wood category). (Format: Categorical)
Categories:
Wood
MDF
Plastic
Metal
Other
N/A
Unknown
Stock Dimensions: length, width, thickness (stock_length, stock_width, stock_thickness): Records the
stock dimensions, in inches, in descending order of size for length, width, and thickness, respectively.
Therefore, these variables record the stock dimension without considering the type of cut being made.
If ranges were provided, the smallest measurement is recorded. (Format: Numerical, Continuous)
50
Includes splitters.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

59
Type of Cut (cut_type_all): Indicates the type of cut, in relation to the stock (not the method of being
cut), being made at the time of the incident. This variable summarizes the more detailed coding found
in the “cut_type” and “other_cut_type” variables. (Format: Categorical)
Categories:
Through/rip
Through/cross
Through/other
Non-through/rip
Non-through/cross
Non-through/other
Unknown/rip
Other (specified in “other_cut_type”)
N/A
Unknown
Personal Protective Equipment (operator_safety_all): Identifies the type of safety clothing and other
gear the victim wore at the time of the incident. This variable summarizes the more detailed coding
found in the “operator_safety1,” “operator_safety2,” and “operator_safety3,” and “other_op_safety”
variables. (Format: Categorical)
Categories:
None
Eyeglasses
51
Safety glasses/goggles
Other
Multiple
Unknown
51
Eyeglasses was an option to this category in the data record sheet of the IDIs. CPSC staff does not endorse
eyeglasses as safety gear, but distinguishes between eyeglasses and safety glasses/goggles.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
60
Tab B
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

UNITED STATES
CONSUMER PRODUCT SAFETY COMMISSION
4330 EAST WEST HIGHWAY
BETHESDA, MD 20814
Memorandum
61
Date:
November 13, 2018
TO :
Caroleene Paul, Table Saw Project Manager
Division of
Mechanical and Combustion Engineering
Directorate for Engineering Sciences
THROUGH :
Alice M. Thaler, DVM, Associate Executive Director
Directorate for Health Sciences
Jacque Ferrante, Ph.D., Director
Division of Pharmacology and Physiology Assessment
Directorate for Health Sciences
FROM :
Jason R. Goldsmith, Ph.D., Physiologist
Division of Pharmacology and Physiology Assessment
Directorate for Health Sciences
SUBJECT :
Table saw blade-contact injuries
In support of the notice of proposed rulemaking to develop a mandatory standard for safeguards
against severe injuries from table saw blade contact, CPSC staff conducted a follow-up special
study on table saw blade-contact injuries that occurred during calendar year 2017. The purpose of
the special study was to gather more accurate estimates of the hazard patterns, including the types
of saws involved and the blade-contact injuries that were received. The special study consisted of
follow-up in-depth investigations (IDIs) of the incidents involving consumers who suffered
emergency room-treated table saw blade-contact injuries between January 1, 2017, and December
31, 2017, that were reported through the National Electronic Injury Surveillance System (NEISS).
During the review of the completed IDIs, the CPSC staff subject matter experts review team
(“review team”) observed that the NEISS injury diagnosis code did not always accurately reflect
the type, extent, and/or severity of the blade-contact injuries incurred (in part, because diagnosis
codes do not exist for all types of injury); in some cases the diagnosis code was entirely incorrect.
Medical records were available for only 6 percent of the 161 incidents, and photographic evidence
of the injuries was available for only 31 percent of the 161 incidents. However, in some cases, the
review team determined that the diagnosis recorded in NEISS was inaccurate or inappropriate and
that a different injury diagnosis better characterized the injuries. This determination was based on
review of medical records, when available; written narratives; survey responses; NEISS final
disposition codes; and photographic evidence, when available.
In this memorandum, Health Sciences (HS) staff discusses the findings of the analysis of the 2017
NEISS data in terms of the injury diagnoses and provides the reasoning for the review team’s
decision to change injury diagnoses in some cases to more accurately characterize the injuries.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

62
The memorandum is divided into three sections. The first section provides an introduction to the
anatomy and physiology of the digits, which is the anatomical location of the vast majority of the
table saw blade-contact injuries. This section provides a detailed description of the various
constituent tissues found in the digits and serves as the foundation for the discussion in the second
section of the blade-contact injury potential to these tissues. Organized by the depth of cut, the
second section outlines how each tissue type is likely to be injured and discusses what treatment,
if any, is required for healing to occur. Building on the first two sections, the third section
discusses the findings of the review team’s analysis with regard to the injury diagnoses. The
various classes of incidents, for which a change in the diagnosis code was necessary, are described
and the reasoning behind making these changes is explained.
1. Anatomy and Physiology of the Digits
The five digits, colloquially referred to as the thumb, index, middle, ring, and little fingers,
respectively, are articulating appendages of the hand that allow one to grasp, touch, and sense
objects in the environment. The thumb and index finger are uniquely positioned to perform
independent movements that exceed those of the other three digits, and can also work in concert
to perform fine motor motions, including prehensile movements, which require the opposition of
thumb to index finger, such as grasping or picking motions. (As will be seen in the third section,
these are also the two digits that are most often injured in table saw blade-contact injuries.) The
essential structures that support these functions include bones, tendons, nerves, a hard nail, a
spongy pad, and a generous vascular system. The anatomical and physiological overview provided
in this section is intended to highlight the complexity of these structures and their close proximity
to one another, and to provide an understanding of how and why the digits are highly vulnerable
to blade-contact injury that can result in serious, permanent impairment.
This section will begin with an overview of skin characteristics. It will be followed by tissue-
specific descriptions that begin at the volar (palm side) surface of the digit and move upwards
through the digit to the dorsal surface (top side); this track will start with the most superficial
tissues and progress toward the deepest tissue, the bone, and then proceed toward the more
superficial tissues on the dorsal side of the digit. Where applicable, notable age and sex differences
are discussed.
General properties of the skin
The skin is a dynamic tissue that is tough, but also soft and pliable (Marble, 1960). It represents
the interface between the body’s external and internal environment. When intact, it provides
protection against mechanical trauma, dehydration, noxious chemicals, thermal injury, bacteria,
viruses, liquids, and ultraviolet radiation (Marble, 1960; Wysocki, 1999; Trott, 2005; Rayan and
Akelman, 2011). Via its rich vascular supply and many sweat glands, the skin helps regulate body
temperature. The skin also possesses the sensory receptors of the nervous system that allow us to
perceive pain, pressure, temperature, touch, and vibration. The skin produces protein in the form
of hair and nails, oils, water in the form of sweat, and vitamin D (Marble, 1960).
The skin is composed of two distinct layers: the epidermis, the outer layer, which we see, and the
underlying dermis. The thickness of the skin and its component layers are the subject of
considerable ambiguity in the medical literature, with some authors providing values that vary
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
63
greatly from those cited by others. In part, this appears to be due to differences in the areas sampled
and/or the tissues that are considered to be part of the skin, but also appears to be due to the
methodology employed to make such measurements. Measurement techniques have included
measuring the thickness of skin folds, microscopically examining sectioned skin, radiography, and,
more recently, ultrasound. The ultrasound technique has been continuously refined and appears
to have allowed for the most precise measurements.
In general, the thickness of the skin has been found to vary throughout the body (Southwood, 1955;
Goldsmith, 1983; Fornage and Deshayes, 1986; Wysocki, 1999; Rayan and Akelman, 2011).
Recent sonographic analyses of the skin have concluded that skin thickness increases at puberty
and starts to become thinner again after the second decade (Tan et al., 1982; de Rigal et al., 1989;
Seidenari et al., 1994). Skin thickness is also known to increase as a result of exposure to the sun
(Richard et al., 1994). In general, the skin of men is thicker than that of women (Southwood, 1955;
Alexander and Miller, 1979; Tan et al., 1982; Fornage and Deshayes, 1986; Seidenari et al., 1994).
Aged skin (the skin of someone in at least their sixth decade) is atrophic (in a state of deterioration),
making it transparent and less elastic, and allowing the vasculature to become more apparent
(Montagna and Carlisle, 1979; de Rigal et al., 1989; Gilchrest, 1996). In addition to a thinning of
both the epidermal and dermal layers with aging, the junction between the layers flattens, making
the skin more fragile (Gilchrest, 1996; Baumann, 2007). A decrease in the vascularity of the
dermis with aging and a reduction in the activity of fibroblasts (see below) results in prolonged
wound healing (Gilchrest, 1996).
The thinner and more superficial of the two skin layers, the epidermis (also called the cutaneous
layer), serves as the body’s first line of defense against injury. It is avascular (lacking blood
vessels) and contains no nerve endings; it is dependent on the underlying dermis for both nutrition
and oxygen (Marble, 1960; Wysocki, 1999; Trott, 2005). The epidermis is a stratified epithelium
that is made up of four or five layers (depending on its location in the body). In a constant state
of turn-over, cell division occurring at the deepest level results in the migration of cells outward,
eventually reaching the outermost layer over a period of weeks, where they are ultimately shed to
the environment (Goldsmith, 1983). The majority of the cells that make up the epidermis produce
the protein keratin. When cells reach the surface, engorged with keratin, they eventually die.
Between the epidermis and dermis is a thin basement membrane, essentially a firm mesh of fibers
(Marble, 1960). Directly below, and attached firmly to the basement membrane, is the dermis,
which is also called the cutis. The dermis represents the next line of defense against injury to the
skin. It is both vascularized and innervated, providing both the blood vessels and nerves that
supply the epidermis; the red or blue hue of the skin arises from this layer and the amount of
oxygenated, versus deoxygenated, hemoglobin within the vascular network (Marble, 1960;
Wysocki, 1999). In addition to sensory nerve endings, the dermis contains hair follicles, sweat
glands, sebaceous glands, and lymphatics.
The dermis is many times thicker than the epidermis and represents the majority of the thickness
of the skin. Unlike the epidermis, the dermis contains few cells; its thickness is due to connective
tissue rather than cells. The main cell type found in the dermis is the fibroblast, which produces
both collagen and elastin (Wysocki, 1999). Collagen is the principal structural component of skin
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
64
and provides the skin with both tensile strength and elasticity, whereas elastin is responsible for
returning the skin to its normal configuration after it is stretched or pinched (Wysocki, 1999; Haake
et al., 2004). The dermis is essential for proper wound repair; the fibroblast cells, and other cell
types found in the dermis, such as macrophages, mast cells, and lymphocytes, are active during
wound healing (Trott, 2005).
The aged dermis is relatively acellular and avascular, and is also characterized by both altered
collagen production and the development of fragmented elastic fibers that results in a large
decrease in its overall thickness (Baumann, 2007). The decreased tensile strength of the dermis
diminishes its ability to resist injury and also makes sutures placed in this tissue less effective; in
people over approximately age 50, sutures placed in the dermis tend to tear the tissue (Trott, 2005).
Skin – volar surface
The skin covering the digits is adaptively different than that of other areas of the body. The skin
found on the volar surface of the digits is thickened, lacks hair, and possesses both whorls
(fingerprints) and flexion creases. This specialized skin is termed glabrous skin. In the digits, the
thickness of the skin varies from one surface to another; this is due to differences in the thickness
of the epidermis and dermis (Southwood, 1955; Goldsmith, 1983; Fornage and Deshayes, 1986;
Wysocki, 1999; Rayan and Akelman, 2011).
The epidermis in the digits ranges from 0.3 mm to greater than 1.0 mm in thickness (Southwood,
1955). On the volar surface of the digits, the epidermis is approximately 0.5 - 0.7 mm thick;
whereas, on the dorsal surface of the digits, the epidermis is only 0.3 mm thick (Moore et al., 2003;
Rayan and Akelman, 2011). Southwood (1955) found age- and sex-related differences in
thickness of the epidermis in samples taken from the digits; the thickness grew from approximately
0.4 mm in infancy to 0.7 mm in the teenage years of puberty, followed by a decline after
approximately age 40, achieving a thickness of approximately 0.5 mm nearing age 70.
Additionally, the thickness of the male epidermis was overall found to be greater than that of the
female by as much as 0.1 mm up to at least the fourth decade, after which differences diminish to
only hundredths of a millimeter (Southwood, 1955).
In the digits, the dermis is approximately 1.4 mm thick on the volar surface (Southwood, 1995)
and 1.5 mm thick on the dorsal surface (Moore et al., 2003). The relative age-related changes in
dermal thickness and overall thicker dermis in men were found to be similar to those for the
epidermis.
Subdermal Fascia – volar surface
Below the dermis are two layers of fascia (connective tissue), the superficial fascia and the deep
fascia. Some medical experts consider these fascia layers as part of the skin, and this may, in part,
account for the disparity in the values reported for skin thickness. The superficial fascia, which is
also known as the subdermis or hypodermis, lies directly below the dermis. It is comprised of
loose connective tissue that provides a supportive base to the skin, attaching it to underlying
structures, and enclosing varying amounts of fat (Wysocki, 1999; Agache and Humbert, 2004;
Trott, 2005; Rayan and Akelman, 2011). This tissue insulates the body against heat loss, provides
a minimal amount of protection against trauma, and is responsible for an individual’s particular
body shape (Wysocki, 1999). Although structurally similar to the dermis, the connective tissue of
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
65
the superficial fascia is looser (Agache and Humbert, 2004; Trott, 2005). The blood vessels and
sensory nerve branches that innervate the skin course through this fascia, just below the surface of
the dermis. Pacinian corpuscles (mechanical pressure transducers) are also located within this
tissue (Agache and Humbert, 2004).
In the digits, the superficial fascia of the volar surface is a specialized structure that plays a
significant role; it is a thick tissue layer that is highly developed and is referred to as the digital
pulp. The pulp space of the digital tip (fingertip) is composed of collagen fiber cords and a
branching vasculature. Collagen fibers, called septa, that radiate out from the skin in spoke-like
fashion, attach the dermis to the tissue surrounding the fibrous tendon sheath (sheath that surrounds
the tendon) and periosteum (the connective tissue that envelopes the bone), providing a firm
attachment of the skin of the digit and digital tip to the bone (Rayan and Akelman, 2011). These
structures also anchor the fat and prevent the skin from sliding during movements of the digits.
The lobules of fat found between the radiating collagen fibers within the pulp space provides
elasticity to the digital tip.
Both the bone and the fingernail provide support to the pulp space. The digital pulp acts like a
compression pad, similar to the fatty pad found in the palm of the hand or in the heel of the foot
(Murai et al., 1997); it distributes the loads when pressure is applied to the tip and allows for
pinching and grasping maneuvers, as well as for tactile sensation. The septa are also important in
injury or infection, because they act to restrict both the amount of swelling and spread of infection
that can take place in the digital tip (Rayan and Akelman, 2011). Injuries to the pulp space can
lead to loss of function and sensitivity, and to persistent pain (Murai et al., 1997).
As described by Doyle (2006), the digital tip
“...represents a complex functional unit that consists of bone and soft tissue in the form of
thick skin that covers a fat pad with fibrous tissue elements that separate the fat into
compartments. This complex structure includes nerves and specialized end organs that
provide sensibility to the digital tip in the form of pressure, pain, temperature, and
identification of form and texture.”
Together with the skin and other soft tissue, including the flexor tendon (see Flexor tendons below)
and its sheath, the pulp underlying the volar surface represents approximately 56 percent of the
volume of the digital tip. The remaining volume consists of the dorsal soft tissue (approximately
26 percent) and bone (approximately 18 percent; Murai, et al, 1997).
The deep fascia is a thick and dense fibrous tissue layer that acts as a base for the superficial fascia;
it also protects the underlying soft tissue structures, providing a barrier against the spread of
infection from the skin and superficial fascia into the underlying soft tissues (Trott, 2005).
Flexor tendons
Tendons are cords of tough, inelastic connective tissue composed of collagen, through which the
power of muscle contractions are transmitted to the digits. The tendons that are responsible for
flexion of the digits (e.g., when grasping items or making a fist) are located in the superficial fascia.
The thumb has one flexor tendon, whereas the remaining digits have two main flexor tendons, the
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
66
flexor digitorum profundus and flexor digitorum superficialis, each occurring in a pair (Trott,
2005). The profundus provides the power needed for gripping and runs deep to the superficialis
on its way to the fingertip, but at the level of the middle phalanx (middle bone segment) in digits
2 through 5, it passes through the superficialis and attaches to the distal (further away from the
body) phalanx. The superficialis tendons are responsible for the positioning of the digits that is
necessary for flexion. They are located superficially, just superficial to the dermal layer, until they
are split by the profundus at the location of the middle phalanx at which point they course deeper
and attach to the proximal (closer to the body) portion of the middle phalanx (Trott, 2005). The
muscles to which these tendons are attached are located in the forearm; the digits themselves are
devoid of muscle tissue.
The tendons are enveloped within a double-walled, synovial fluid-filled sheath that both lubricates
and nourishes them (Marble, 1960; Rayan and Akelman, 2011). The inner layer is highly
vascularized, has many tendon cells, and is rich in collagen. It closely adheres to the flexor tendon
and is essential for the gliding, nutrition, and healing of the tendon. The outer layer of the sheath
is surrounded by fibrous thickenings that are referred to as pulleys. The pulleys allow the muscles
in the forearm to transform small movements of the tendons into a large amount of torque at the
joints, which is necessary for pinching and grasping (Rayan and Akelman, 2011).
Digital nerves
There are two digital nerves that innervate each digit. The digital nerves travel along the radial
(toward the thumb) and ulnar aspect (toward the little finger) of the volar surface of the digit within
a neurovascular bundle (containing both nerves and blood vessels), and move ventral and lateral
to the flexor tendons (Trott, 2005). The nerves arborize at the base of the nail, forming a network
of sensitive nerve endings with branching occurring both upwards and downwards within the digit
and providing sensation to both the nail bed area and volar surface of the digit and digital tip
(Marble, 1960; Trott, 2005; Rayan and Akelman, 2011). The digital tip also possesses glomulus
bodies, which are neurovascular structures composed of intertwined nerves and blood vessels that
regulate blood flow at the perionychium (the nail unit; see Nail below); they are found within the
nail bed and throughout the digital tip (Rayan and Akelman, 2011).
Blood Vessels – volar surface
Each digit has two digital arteries, radial and ulnar, that travel alongside the digital nerve on the
volar side within the neurovascular bundle, just slightly deep to it within the superficial fascia
(Rayan and Akelman, 2011). Proximal to the proximal interphalangeal joint (see Bone below),
the digital arteries bifurcate, sending a dorsal branch to the skin on the dorsal side of the digit.
Similar to the branching of the nerves that occurs at the base of the nail, the blood vessels also
branch out just proximal to the nail root, toward both the dorsal and volar sides of the digit. The
tip of the digit is richly vascularized with end loops formed by capillaries in the digital pulp (Rayan
and Akelman, 2011). The venous return in the digits consists of a superficial and deep set of veins.
Deep veins run alongside the digital arteries.
As stated by Trott (2005), the hand possesses a circulation that is both rich and redundant. Relative
to other parts of the body, the hand receives a relatively greater blood supply, and the supply to
the distal phalanges (bone segments) is greater than that to the other phalanges (Marble, 1960).
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
67
Based on that, and the fact that the circulation to the bone is relatively small, Marble reasons that
the majority of the blood going to the digit supplies the skin.
Bone
The thumb is composed of two phalanges, the proximal and distal phalanx, which are separated
by one joint, the interphalangeal joint. The remaining four digits are each composed of three
phalanges; the proximal, middle, and distal phalanx. Between the proximal and middle, and
middle and distal phalanx of these four digits are the proximal interphalangeal joint and the distal
interphalangeal joint, respectively. Each segment of a given digit is named for the underlying
bony phalanx (e.g., the terminal segment of the middle finger is referred to as the distal phalanx).
Retaining Ligaments
Ligaments are tough tissues that act to hold together the bones of a joint. Like tendons, ligaments
are also formed from collagen, but their bundles are less regular (Marble, 1960). At the
interphalangeal joints, two ligaments attach the skin to the underlying tissues. Both of these
fibrous tethers extend from the one side of the digit to the other, one traveling dorsal to the
neurovascular bundle and one traveling beneath it, closer to the volar surface. These ligaments
stabilize the joint, positioning both the skin and neurovascular bundle during movement of the
joints (Rayan and Akelman, 2011).
Blood Vessels – dorsal surface
The digital arteries that run along the dorsal side of the digit travel in the superficial fascia and
branch at the distal interphalangeal joint. The dorsal veins, which are also found in the superficial
fascia, superficial to the extensor tendons, are part of a larger system than the deeper venous system
(Rayan and Akelman, 2011).
Subdermal Fascia – dorsal surface
The deep fascia of the dorsal aspect of the digits is a layer of tissue that both incorporates and
binds the extensor tendons. This layer contains sensory nerves as well as the venous return from
the skin (Rayan and Akelman, 2011). The superficial fascia on the dorsal surface is a very narrow
layer of loose connective tissue and a small amount of adipose tissue. It is loosely attached to the
dermis, permitting the skin on the dorsal surface to move freely as the digits are flexed. Coursing
through this fascia are the veins of the superficial venous system (Rayan and Akelman, 2011).
Nail
The most prominent feature on the dorsal surface of the digits, the nail plate (fingernail) is part of
a complex structure, called the perionychium (or nail unit), which is composed of the nail bed and
the paronychium, the surrounding soft tissue that envelopes the nail along its lateral margins
(Zook, 1990). The integrity of the perionychium is essential for the proper growth, tactile touch,
regulation of peripheral circulation, as well as protection of the digital tip (Zook, 1990; Rayan and
Akelman, 2011). Due to its location at the tip of the digit, the nail unit is particularly vulnerable;
per Rayan and Akelman (2011), it is the part of the hand that is most frequently injured.
The nail plate is the hard, visible portion of the nail and is composed of a keratinous material that
remains after the death of the cells from which it is initially formed (Rayan and Akelman, 2011).
The nail plate varies in thickness from about 0.6 to 1.0 mm and grows at a rate of 0.1 mm per day
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
68
(Levit and Scher, 2004). The nail plate is devoid of cells in all but the area of the lunula, the white
hemispherical (crescent moon) shape at the base of each nail; the absence of nuclei in these cells
allows for the transparence of the nail plate. The normally pink coloration of the nail plate distal
to the lunula is due to the underlying vascular system, which is seen through the nail plate (Zook,
1990).
The nail plate increases sensitivity of the digital tip by allowing the digital pulp to be compressed
between it and what is being touched; consequently, the sensory nerve endings within the pulp are
better able to discern what is being touched (Zook 1990; Rayan and Akelman, 2011). Removal of
the nail results in reduced touch sensation, due to a significant increase in the two-point
discrimination distance (Zook, 1990), i.e., the minimum distance between two objects that is
necessary to discern them as distinct from one another.
The nail bed, which the nail plate sits upon and adheres to, is a soft tissue consisting of the germinal
matrix and the sterile matrix. The germinal matrix lies under the base of the nail (nail root) and is
where new nail is generated; the cells forming this matrix are the source of the majority of the cells
that make up the nail plate. The germinal matrix begins proximal to the visible portion of the nail
and extends to the lunula (Zook, 1990; Rayan and Akelman, 2011). The deepest layer of cells
making up the germinal matrix rests directly on the periosteum of the distal phalanx; consequently,
fractures of the distal phalanx may disrupt this delicate tissue and, ultimately, the proper growth
of the nail plate (Zook, 1990; Rayan and Akelman, 2011).
The sterile matrix adheres to the periosteum of the distal phalanx and is located distal to the
germinal matrix. This matrix contributes a thin layer of cells to the deepest portion of the nail
plate and increases its adherence to the nail bed; the actual amount varies by the individual, and,
in some, can be so little that the nail is less tightly adhered (Zook, 1990). This matrix is the tissue
that the nail plate passes over as it grows from the base of the nail toward the tip of the digit. As
the nail plate moves forward, so too do the cells of the nail bed (Wood and Bladen, 1985).
Deformities of the nail bed, such as ridging, can result when this tissue is injured or deformed
(Zook, 1990; Rayan and Akelman, 2011).
The nail fold is the socket of tissue that anchors the proximal portion of the nail plate in place; its
floor is comprised of the germinal matrix and its roof is comprised of the terminal portion of the
eponychium, a specialized soft tissue that is located proximally to the nail, a portion of which (the
cuticle) overlays the nail (Wood and Bladen, 1985; Zook, 1990; Rayan and Akelman, 2011). The
skin that frames the nail plate along its sides (paronychium) functions to both stabilize the nail and
prevent infection from developing under the nail (Rayan and Akelman, 2011). The hyponychium
is the keratinous skin under the tip of the nail where the digital pulp meets the sterile matrix; this
thickened epidermis is both highly vascularized and innervated (Wood and Bladen, 1985; Rayan
and Akelman, 2011).
Extensor Tendons
The thumb has two extensor tendons. The remaining digits each have a main extensor tendon that
powerfully extends the digits and a small accessory tendon that can extend the digit in a weak
fashion when the main extensor tendon is compromised (Trott, 2005). The extensor tendon inserts
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

69
into the distal phalanx just proximal to where the germinal matrix is located. All the extensor
tendons are very superficial and may be apparent when one extends the digits.
Skin – dorsal surface
As already noted, the skin on the dorsal surface is thinner than the volar surface. Unlike the
glabrous skin of the volar surface, the skin on the dorsal surface bears hair follicles, is relatively
sparsely populated with sensory nerve endings, is found in excess over joints, and is more mobile
than the skin on the volar surface (Rayan and Akelman, 2011).
With an appreciation of the many tissues that make up the complex structure of the digits, it is now
possible to discuss how these tissues may become injured as a result of contact with a table saw
blade.
2. Table Saw Blade-Contact Injuries
Given the operating characteristics of a table saw and the attributes of a typical table saw blade, it
is exceedingly likely that someone who contacts the spinning blade will suffer, at a minimum, a
disruption of the skin (i.e., receive at least a minor laceration injury). This is borne out by the 161
incidents in the 2017 NEISS dataset that were reviewed, all of which resulted in some form of
laceration injury; there was an absence of (less severe) abrasion or contusion injuries (such injuries
could occur, particularly if contact was made with only the plate of the blade rather than its teeth).
Unfortunately, many who are injured by a table saw blade will suffer far worse than just a break
in the skin. Such more severe wounds can involve all layers of the skin and damage to the
underlying structures, and require extensive, long-term, complicated wound management,
including multiple surgeries, long recuperation times, and the need for physical rehabilitation.
Furthermore, these wounds and their treatment may be extremely painful, and may leave the victim
badly scarred, disfigured, functionally impaired, and psychologically traumatized (Mason et al.,
2002).
Practically speaking, all table saw blade-contact injuries are some form of a laceration injury, the
depth, width, length, and severity of which can fall anywhere along a very wide spectrum,
depending on a host of factors that include: (1) the angle and speed of approach of the hand/digits
(i.e., movement of the hand across the blade vs. directly into the blade; rate of approach/feed rate),
(2) the height and angle of the saw blade, (3) the rotation rate of the blade, (4) the thickness of the
blade, (5) the condition of the blade, (6) the number, type, and configuration of the teeth, (7) the
angle at which the teeth are set relative to the center of the blade, (8) the metal composition of the
teeth and their condition, (9) the condition of the bearings, (10) the number of digits affected, (11)
the location along the length of the digit(s) where contact is made, and (12) the underlying
structures that are ultimately contacted by or affected by the teeth of the blade.
At one extreme, blade contact can produce shallow, minor lacerations that disrupt only the skin.
Injuries such as these may require little to no medical attention, are relatively inexpensive to treat,
and likely will have no lasting repercussions. The width of the swath and/or the length of the
laceration may necessitate the application of sutures to aid wound closure and healing. An
exception to the injury potential of such shallow wounds is a laceration that involves the nail plate;
such injuries can require extensive surgical repair, and even in the best of circumstances, result in
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
70
deformities of the nail plate and/or a compromised ability to touch and grasp due to a deformed
nail plate (see Severe lacerations below for discussion of nail plate injury).
Table saw blade teeth that penetrate only slightly deeper (i.e., greater than approximately 4 mm
from the skin surface) than those producing minor lacerations, have the potential to produce
injuries that can be far more severe and both complex and expensive to treat. This is owing to the
many tissue types found in the digits (as described in first section), their close association to one
another, and their close approximation to the skin layers under which they lie. Saw blade teeth
that penetrate to such depths can easily lacerate the subdermal fascia, tendons, and the bilateral
neurovascular bundles that traverse the length of the digits and house both the nerve and vascular
supply of the digits. Still deeper penetration of the blade can injure ligaments and bone. The
complex laceration of nerves, blood vessels, tendons, ligaments, and bone are severe lacerations
that will require extensive and complicated surgical treatment, including microsurgery to
reestablish nerve connections and restore blood flow to the injured digit, surgery to reconnect
tendons and repair ligaments, and the resetting of bone.
Amputation injuries are an extension of the most severe lacerations – differing only by the fact
that the laceration proceeds all the way through the thickness of the digit, separating the digit from
the hand, or segment of the digit from the remainder of the digit. Depending on the location and
condition of the amputated digit/segment, the treatment may be very similar to that required for a
severe laceration, but may also necessitate the surgical shortening of the digit, the replanting
(reattachment) of the amputated segment, the application of skin grafts, or the complete removal
of the digit.
In general, the injury severity will determine whether the wound from a table saw blade can be
allowed to heal on its own (healing by secondary intention) or will require medical treatment that
may include surgical closure of the wound (healing by primary intention). Given the complexity
of the digits and the unique attributes of the component tissues, the likely table saw blade-contact
injuries that may occur will be discussed in greater detail below; discussion will start with the most
superficial of injuries and proceed to those involving the deepest structures. Special emphasis will
be placed on the unique properties of the tissues affected, the required wound treatment, and the
long-term consequences of such injuries.
Simple laceration injuries and avulsions, not involving deeper structures
As mentioned above, laceration injuries can be divided into simple lacerations, complex
lacerations, and those that completely sever the digit, i.e. amputations. Simple lacerations are, for
the most part, minor injuries, which involve only the skin layers. These injuries may heal without
any intervention, or require only minor care, such as cleaning and applying dressing to the wound,
thereby allowing it to heal spontaneously, or may require primary surgical closure (healing by
primary intention) in the emergency department in order for healing to occur.
The shallowest of cuts will penetrate only the epidermis. Given that the epidermis does not possess
any blood vessels, there is no bleeding in such wounds; a paper cut that does not bleed is an
example of such an injury. Such wounds only require a few days to heal. New cells are formed
and they migrate to fill in the wound. Because the epidermis is so thin, when examining a wound
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
71
it cannot be easily differentiated from the dermis with the naked eye alone; however, the absence
of blood will confirm that only the epidermis has been affected.
Slightly deeper lacerations will also injure the dermis. Wounds of this depth will take several days
or weeks to heal completely. In general, there are several phases to healing from this type of
injury. The immediate response is one of rapid hemostasis. Severed blood vessels will initially
flood the wound with blood, which will clean the wound of microbes and other contaminates.
However, such bleeding will be limited due to wound-edge retraction and tissue contraction, which
compresses the small vasculature, and reflex vasoconstriction. The exposed wound surfaces will
begin to amass platelets, which will fill the wound with clotting material, the top of which will
harden into a scab (Falabella and Falanga, 2004; Trott, 2005). Other compounds released into the
wound will result in the dilation of uninjured capillaries, which will initiate the flushing of the
wound of bacteria and contaminants (Wysoki, 1999; Trott, 2005).
The next phase is the inflammatory response, wherein granulocytes and lymphocytes (both forms
of white blood cells) are attracted to the wound to mitigate bacterial infection. Within a day or
two, macrophages (also a form of white blood cell) appear in great numbers and digest debris in
the wound and also stimulate fibroblast reproduction and the growth of new blood vessels
(Trott, 2005). Simultaneously, intact cells of the basal layer of the epidermis begin to form foot-
like structures and combined with their accelerated replication, will begin to fill in the wound over
the damaged dermis and under the scab, and reestablish the normal layering of the epidermis (Trott,
2005).
Within a few days, new blood vessels will replace damaged vasculature, which sustains the wound
healing process. This, in turn, promotes the proliferation of fibroblasts and the production of new
collagen fibrils, which are laid down in a random pattern, having little tensile strength (Wysocki
1999; Trott, 2005).
Over weeks and months, the collagen is continually broken down and replaced, forming a stronger
tissue as time progresses. As new tissue and blood vessels grow beneath the scab, filling in the
damaged area, the initial blood clot is replaced. The scab falls off once cells in the epidermis have
regenerated. A scar, which is composed mainly of collagen, usually remains. The scar tissue has
little or no blood supply and has less flexibility than normal skin.
Over many months, the scar will undergo remodeling, contracting toward the center point of the
wound as it does so, which pulls the surrounding normal skin into the wound area. Wide wounds
and those involving significant surface area will eventuate in noticeable scarring; whereas, deep
wounds that cause injury to underlying structures will be depressed or otherwise irregular
(Trott, 2005).
Some wounds will require intervention for proper healing to occur. To make the determination
whether it is necessary to repair the tissues and close the skin with the placement of sutures, to
close the wound without repairing it, or to leave it open, debris must be removed from the wound
and it should be cleaned and debrided (all contaminated and dead tissue removed) before
attempting to match up the sides of the wound (Marble, 1960). Sutures may be required if the
tissues do not lie closely opposed or if the laceration is lengthy. Per Wittstadt (2005), primary
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
72
closure is straightforward and will result in good sensation, rapid healing and early mobilization.
Closure of this type is appropriate for lacerations that are relatively clean and with minimal tissue
loss (Trott, 2005).
Given the critical function that the skin plays in the digits, the only skin edge that should be excised
during treatment of laceration injuries is that skin which is clearly mechanically damaged.
Excessive loss and/or removal of skin is problematic, and can lead to inadequate coverage or
wound contraction (Marble, 1960; Trott, 2005). Excision of dermal tissue should be done
sparingly and limited to only that tissue that is compromised, as any defects in the dermis are
replaced by scar tissue (Marble, 1960; Trott, 2005). The edges of the injured skin should be
cleaned down to the pink tissue. Marble cautions that in a simple laceration, the damage to the
skin is slight and excision of the edge is unlikely to be necessary and should rarely be done, as
there is no excess skin on the hand and that any loss, no matter how small, must be replaced with
skin grafts from other parts of the body. The laceration created by a table saw blade is likely to
require a greater amount of excision. If grafting is necessary to close the skin, there should be no
tension, because tension will affect healing. Open treatment (healing by secondary intention) is
often reserved for children and for injuries of moderate size (1 cm squared or less; Wittstadt, 2005).
Avulsion (forceful tearing away) injuries of the skin can also occur under certain circumstances
after contact with a table saw blade and can be minor or severe, depending on the size or volume
of the tissue that is torn away. There is agreement that fingertip avulsions that are less than 1-cm
square in area and with no bone exposed can be left to heal spontaneously (Trott, 2005).
Individuals with older, thinner skin are more likely to suffer partial avulsions of skin to forces that
would not disrupt younger, thicker skin. In such cases, the skin separates at the boundary between
the dermis and superficial fascia. Unfortunately, slower wound healing also occurs in those of
advanced age (Trott, 2005). When the protective skin layers are stripped from any part of the
hand, fascia, tendons, blood vessels, nerves, ligaments, bones and joints can be revealed. If not
promptly covered, these tissues can become dry, infected, and die; thus, any loss of skin must be
promptly replaced (Marble, 1960).
Avulsions of the nail plate can also occur. If cleanly avulsed from the nail bed, very little treatment
is necessary. However, when greater injury of the nail unit is produced, or the avulsion occurs
along with laceration of the underlying or supportive tissues, then the injury may be more severe
and require more complicated treatment (see Severe lacerations, fractures, and avulsions,
involving deeper structures below for discussion of nail plate injury).
Severe lacerations, fractures, and avulsions, involving deeper structures
What outwardly may appear to be a minor laceration injury can actually be much more serious
when underlying structures have been compromised; however, the detection of these more
extensive injuries may not occur until the wound is opened further and an elaborate inspection is
performed. Thus, treatment of anything but the most minor laceration wound from table saw blade
contact should involve inspecting the deeper tissues to determine the true extent of the injury.
As described by Loda (1999), injuries of the digit, and the tip in particular, can be totally disabling.
This is because of the very precious digital sensitivity of the digits. Recognition of the extent of
the injury and receiving the proper treatment are of critical importance in regaining sensitivity.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
73
Loda cautions that recovery from an injury to a digit can be thought of in either terms of basic
recovery or functional recovery. Basic recovery consists of the restoration of nerve pathways and
simple reception of touch, cold, heat and pain, whereas functional recovery describes the ability to
recognize an object, assess it, and intellectually interpret what it is. Any modification to the
sensitivity of the digits will also affect their functional ability. Thus, it is essential that the true
extent of a blade-contact injury be carefully assessed.
The action of the table saw blade is one that both crushes and compresses the tissue as it lacerates
through the tissue; consequently, the tissues that are affected may lie deeper than the actual
penetration depth of the teeth of the table saw blade. If it is apparent that the deeper structures
have been involved, Furlong (1957) advises that the patient should be admitted to the hospital, so
that the required exploration of the wound is not rushed and any complications can be addressed.
Table saw blade wounds are marked by ragged or shredded edges, with skin and superficial fascia
that are devitalized in the process; these wounds are more susceptible to infection than a more
sharp shearing injury (Trott, 2005). In contrast to the wounds made by a surgeon’s scalpel (incised
wounds), which require little debridement, laceration wounds in general require relatively more
excision of tissue, but those that also involve crushing of the tissue, as occurs with a table saw
blade, require even more (Marble, 1960). Although seemingly obvious, Marble remarks that when
such injuries take place, it should be the surgeons’ goal to ensure that the tendons move, the nerves
transmit, and the bones heal, and describes the necessary techniques as akin to those of the finest
instrument maker. This statement reflects the fact that the digits are complex specialized
structures, where the repair of which must go beyond cosmetic appearance.
Treatment decisions are often based on a combination of the affected anatomy, the orientation of
the laceration, and the location and geometry of the skin and soft tissue that has been lost, as well
as factors such as the patient’s age, occupation, functional needs, and the surgeon’s experience
with the required techniques (Wittstadt, 2005; Doyle, 2006). However, the more severe laceration
injuries that involve damage to the tendons, nerves, and vascular system, are not injuries that the
body can recover from on its own and will require complex and complicated surgery that is best
performed by a specialist.
The fat in the superficial fascia makes this layer of fascia readily recognizable after a laceration
injury. Fascia tissue that is torn or shredded must be removed, and if not shredded can be repaired
with sutures or left open (Marble, 1960). Trott (2005) advises that the fat of this layer can be
removed as necessary because it is a good substrate for bacterial growth, and failure to remove
devitalized tissue, blood clots, and other debris can result in infection. However, there are a couple
of caveats. The septa of the volar surface should be left intact whenever possible because injury
to this tissue can result in the creation of dead space within the digit, and because injured fat does
not regenerate, fat that is lost from the digital pulp can affect the padding that the tissue provides
(Trott, 2005). Laceration injuries of the deep fascia are easily recognizable by the off-white color
of the sheath-like material. Closure of the deep fascia is necessary after injury to reestablish both
the protective and supportive functions of this layer (Trott, 2005).
Careful exploration must be performed whenever the function of the tendons is in question.
Although function may be maintained, after their direct visualization subsequent to exploration,
the tendons may be found to be partially severed (Trott, 2005). If they are crushed or severed, they
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
74
may be retracted and found encased in a mesh of blood clots. When they are cut, the proximal
half will retract due to the pull of the muscle, and can be difficult to find, whereas the distal segment
is usually easy to locate. Similarly, if during examination, the hand is in an orientation that differs
from the orientation during the injury, the lacerated tendon may not be visible in the wound
opening, but rather some distance away from the laceration through the skin (Marble, 1960; Trott,
2005). In these cases, it may be necessary to actively flex and extend the digits and/or enlarge the
wound in order to locate them. As mentioned above, in general, debriding with a scalpel is
necessary to remove all contaminated and dead tissue, including fascia, torn tendons, and skin.
This is of particular importance with regard to the proper movement of the tendons, because any
trace of foreign material that is left in the wound could cause inflammation, which could disrupt
normal function, such as the smooth gliding of tendons (Trott, 2005). Once located, the tendons
must be washed and the wounded ends trimmed, before the ends can be sutured together (Marble,
1960).
In many cases, lacerated flexor tendons may be repaired as late as 3 weeks after injury, but in those
cases where there is extensive tissue destruction or skin loss, injured bone, or excessive
contamination, repair is best performed immediately. Lacerations of the flexor tendons are
routinely referred to a specialist for attention. Trott (2005) cautions that repair of these tendons is
a delicate matter that is fraught with complications; that even under ideal circumstances, including
treatment by a specialist in tendon injuries, the full range of motion is never realized after such
injuries. Splinting of the digits and forearm for a period of four weeks is necessary after repair of
the flexor tendons.
Severed extensor tendons will require a longer period of splinting than that required for flexor
tendons (6 weeks vs. 4 weeks, respectively; Marble, 1960). Per Wittstadt (2005), even after the
best possible repair and cooperation from the patient, the tendons may become adherent to the
tendon sheath and fail to glide smoothly enough to return adequate digital function. Providing that
the adjacent pulleys are intact, the loss of one tendon pulley can be tolerated; however, loss of
more than one pulley results in ineffective operation of the tendon and loss of motion of the joint
(Rayan and Akelman, 2011).
The colocalization of the arteries and nerves in neurovascular bundles is useful in injury
assessment because cases of arterial bleeding will usually indicate that there has been nerve injury
as well, and vice versa (Trott, 2005). When arteries are completely transected, the vessels will
contract and bleeding will stop; however, when only partially lacerated, the vessels cannot close
and bleeding will continue (Marble, 1960). Veins will bleed vigorously until thrombosis occurs
(Marble, 1960). Severed blood vessels should be sutured closed (Marble, 1960). Through the
process of angiogenesis, new vessels grow, migrating toward the wound (Falabella and
Falanga, 2004).
A digit with compromised sensation is a serious disability; therefore, all severed nerves must be
repaired. The best recovery of nerve function is associated with treatment by individuals skilled
in the proper repair of nerve injuries. The nerves may be lacerated, but are rarely crushed or injured
so severely that they cannot be repaired (Marble, 1960). Once the severed ends are located, they
are washed, their ends are recut, and they are brought together; the sheath that contains them is
then sutured together (Marble, 1960; Trott, 2005). Sutured nerves require four weeks of
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
75
immobilization. Marble (1960) states that the nerves within the sheath will regenerate at a rate of
1 mm per day if the suturing is done properly. The number of millimeters from the injury location
to the tip of the digit will approximate the number of days before sensation will be restored to the
tip of the digit. During healing, for approximately 3 weeks, sensory nerves will sprout extensively,
after which autonomic nerve fibers will appear (Metze and Luger, 2004).
A fracture of one of the phalanges is often associated with injury of the tendons, ligaments, nail
plate, or other soft tissue. Lacerated, or otherwise injured bone, should be cleaned, all
contaminants removed using a small chisel or rongeur (a surgical instrument with a sharp-edged,
scoop-shaped cutting tip), and any small bone fragments removed (Marble, 1960). Whenever the
bone is exposed, shortening of the bone may be required in order to close the wound, but the
preservation of the length of the digit should always be strived for; in particular, this is the case
for the thumb (Rayan and Akelman, 2011). The realignment (reduction) of broken or dislocated
bones can usually be accomplished under local anesthesia in the emergency department; however,
some fractures or dislocations may require surgical repair in an operating room. Splinting of the
bone for several weeks, when required, will stabilize the realigned bone and permit faster healing.
Fractures that are nearer to the joint may require splinting or the placement of pins or wires to
properly align the bone.
Displaced closed fractures of the distal phalanx have to be given special attention; they must be
reduced (either with closed reduction and splinting or placement of wires) and stabilized to prevent
injury of the overlying sterile matrix, which, if injured, could result in deformation of the nail plate.
Fractures from table saw blade contact usually result from direct contact with the bone; however,
fractures of the fragile tuft (end) of the distal phalanx may occur due to the forces involved in the
disruption of surrounding tissue. Small fractures of the tuft generally do not affect the strength of
the bone and require little, if any, treatment. Fractures of the phalanges heal quickly, but the
deposition of calcium occurs after the bone is considered solid (Marble, 1960).
Injury of the nail plate or nail bed can be of significant consequence. Injuries to the nail bed may
result in deformity of the nail plate as well as functional disability. Lacerations can be repaired
only after complete removal of the nail plate and the placement of sutures, followed by placement
of the plate back into the nail fold (Fassler, 1996). When the nail has been injured, it is critical to
ensure that the eponychium is not allowed to adhere to the germinal matrix (directly, or by the
build up of scar tissue), because this will impair nail regeneration. If the nail bed has been exposed
(i.e., in cases of nail avulsion), such adherence can be prevented by suturing the detached nail or
some other material in place until new nail growth pushes it out (Zook, 1990; Trott, 2005). It is
also essential that the nail bed is smooth (i.e., it is necessary to close wounds in this area with fine
sutures), or scar tissue will develop and its presence will not allow for the nail to adhere to the nail
bed (Zook, 1990). When there is loss of the nail matrix tissue, treatment is often difficult and is
likely to result in a deformity of the nail plate (Fassler, 1996).
After repair to the deep tissues has been effected, proper skin closure, whether through suturing,
or grafting, is necessary to save exposed tendons, nerves, joints and bone; not doing so will lead
to their necrosing (Marble, 1960).
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
76
Severe avulsions of soft tissues and/or the nail plate can also occur under certain circumstances
and can disrupt the soft tissues in a manner not unlike the above-described severe laceration
injuries. For larger areas, but with intact nail and no exposed bone, conservative treatment can be
attempted, but skin grafts may be necessary (Marble, 1960; Trott, 2005). Larger wounds that are
allowed to heal spontaneously will have a thin layer of epithelium that may prove not to be very
durable (Fassler, 1996). Granulation tissue will form wherever skin has been removed; it provides
the bed for the development of scar tissue, which can both severely constrain movement about
joints and impair sensitivity (Furlong, 1957). For avulsions with involvement of the nail, repair
of the matrix is necessary.
As articulated by Wittstadt (2005), complications of digital injuries are many and include infection,
hook nail deformity, flexion contracture, cold intolerance, altered sensibility, and graft or flap
failure. Although infection may be minimized by adequate debridement of the wound, antibiotics
beyond the usual course are not generally believed to be helpful in the prevention of infection.
Failure to trim the nail bed back to the level of the bone can result in the nail hooking over; the
nail requires the support of the underlying bone. Use of various flaps can result in the inability to
fully extend the digits, owing, at least in part, to the positioning of the digits during the procedure.
Finally, cold tolerance is a particularly common problem, occurring in 30 to 70 percent of digital
injuries; those who suffer loss of the digital pulp have both a 30 to 50 percent chance of cold
intolerance and a 30 percent chance of having altered sensibility.
For many who receive such severe lacerations, the treatment will extend far beyond the initial
hospitalization. Sutures, wires, fixation points for tendon repair, splints, and casts will have to be
removed, x-rays taken, examinations performed, and, in some cases follow-up surgeries
performed. For many, physical therapy will have to be initiated toward the goal of regaining a
useful range of motion.
Amputation injuries
Amputations are severe laceration injuries that have completely severed the digit from the hand or
a portion of the digit from the remainder of the digit (partial amputation). It is important to realize
the subtle difference between a severe laceration injury that severs the skin and all internal tissues,
but leaves intact the skin on the opposite side of the digit from where the blade entered, and the
amputation injury that completely transects the digit. In terms of the NEISS injury diagnosis code
that may be used, only the slightest difference in the depth of laceration – on the order of 0.5 mm
– separates an injury that will be termed a laceration from an amputation.
Although there is much in common between the treatment of amputations and the treatment of the
severe laceration injuries to soft tissues, as discussed above, amputations present both the treating
physicians and patient with a number of difficult challenges, such as the decision whether to replant
an amputated segment, to surgically shorten an amputated digit, or which digit to salvage when
more than one has been amputated. Tissue that has been separated for too long, small pieces of
tissue, or severely damaged tissue may not be salvageable – an unfortunate reality. In some cases,
the best treatment may consist of leaving the amputated digit/segment off, because reattaching it
may impair the function of the hand. Unlike a severe laceration that may involve one or more
tissues, and require some level of expertise to treat, amputations are likely to require the expertise
of one or more specialists, depending on the tissues affected and the decision to replant or not.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
77
Replantation of digits can occur up to a day after the amputation, if the amputated segments were
properly chilled (Doyle, 2006). After the bleeding is stopped, and the wounded tissue, including
the separated segment(s), are cleaned and debrided, the tissues can then be carefully examined,
and the decision to replant made. Amputations that are relatively clean (not jagged) and which
occur at or proximal to the distal interphalangeal joint are considered candidates for replantation
(Wittstadt, 2005). For such amputations, the main objectives are to preserve the digit length, nail
growth capacity, and the fingertip padding, while retaining sensibility and function, and
minimizing pain and recovery time; the maintenance of length must be balanced against a tension
free closure that is well padded, is not painful, and that will provide for pinch and fine motor skills
(Trott, 2005; Doyle, 2006; Rayan and Akelman, 2011). If the portion of the distal phalanx where
the flexor and extensor tendons insert is lost or cannot be preserved, then the distal phalanx is
generally removed because there is no advantage to preserving a small stump of the distal phalanx
if it cannot be manipulated (Fassler, 1996).
Replantation normally consists of shortening and/or fixation of the bone, repairing tendons,
anastomosis of arteries and veins, repairing digital nerves, and ensuring adequate skin coverage
(Doyle, 2006). Urbaniak (1979) describes the order of the many steps involved in replantation as
follows: (1) locate and tag the vessels and nerves, (2) shorten and fix the bone, (3) repair extensor
tendons, (4) repair the arteries, (5) repair the nerves, (6) repair the flexor tendons, (7) repair the
veins, and (8) complete with skin coverage. In some cases, to preserve the length of the digit, a
joint may be fused; this will no longer permit movement about the fused joint. Replantation of a
single digit can take a microsurgeon or team of specialists 3 hours to perform; whereas, multiple
digits can require as many as 20 hours (Urbaniak, 1979).
Survival of a replanted digit/segment is typically over 95 percent (Godfrey et al., 1984). In some
cases, the replanted digit will not have reperfused (have normal blood flow) over a period of a
couple of weeks, and will have to be surgically amputated. Even amongst the best recoveries,
replanted parts are rarely 100 percent functional and many with a replanted digit/segment will
complain of scar tenderness, pain, and discomfort in cold weather, and may have nail deformities
and reduced range of motion.
When replantation does not occur after a partial amputation, the most must be made of the digit
that remains. If bone is protruding from the wound, it will have to be trimmed back with a rongeur
until there is sufficient skin to close over the wound (to minimize tension on the tissues) or a skin
graft will have to be applied (Marble, 1960). Fassler (1996) remarks that there is rarely sufficient
tissue to surgically close such wounds, and when it is attempted, a painful digital tip or death of
the tissue may result. If bone, tendon, or a joint is exposed, then one of several varieties of local
skin flap will be required to cover the area, some of which can preserve sensation and length of
the digit (Burke, 1984). Split-thickness skin grafts are used to promote rapid healing of digital tip
amputations (Doyle, 2006). When full-thickness skin grafting is required, as in larger wounds or
distal tip amputations, the loss of digital pulp is likely to result in a loss of sensory function and
sensitivity to the cold. Exposed nerves will need to be resected (surgically lacerated) about 1 cm
back from the wound; if this is not done, the normal healing process of the nerve will cause
innervation of the scar tissue, which can be chronically painful (Marble, 1960; Doyle, 2006).
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

78
Table saw blade-contact injuries often produce amputations of the tip of the distal phalanx. Such
injuries can be divided into three types. In the first, the amputation is oblique and there is greater
length preserved across the volar surface than the dorsal surface. This type of amputation is the
most straightforward to treat. After shortening of the exposed bone, the wound can be closed by
suturing the volar skin to the nail plate. In the second type, the damage is the opposite of the first
type – the volar surface is more extensively damaged than the dorsal surface; consequently, this is
the most severe type. To close this wound, almost all of the length of the segment will have to be
sacrificed or a flap from the palm will have to be utilized. The third type is an amputation that is
relatively straight across – perpendicular to the length of the digit – causing an equal amount of
tissue loss on the volar and dorsal surfaces. This is a more complicated wound than the first type,
but is not as severe as the second type. If the surface area is greater than 1 cm squared, then a full
thickness skin graft will likely be required. Alternatively, the bone can be shortened and the wound
closed by primary intention, but this will result in a shorter digit; Burke (1984) states that this is
one of the most common procedures performed.
The one exception to the severe nature of amputation injuries is an amputation that results in the
loss of only the distal portion of the distal phalanx (i.e., most similar to the third type mentioned
in the previous paragraph). Although it may appear to be a devastating wound, if there is minimal
tissue loss and no exposed bone, after cleaning and bandaging, the injury may be left to heal
spontaneously (heal by secondary intention); such treatment is often reserved for those wounds
that are no larger than 1 cm squared (Burke, 1984; Rayan and Akelman, 2011). Remarkably, when
fully healed, such injuries often achieve their previous appearance and level of sensitivity.
An amputation injury can have a profound effect on one’s life, affecting not only their physiologic
state, but their mental state as well. The loss or disfigurement that results can produce feelings of
helplessness and may leave the individual feeling incomplete. Some will proceed through the
various stages of grieving as they try to cope with their loss. Others may be affected for some
period of time with phantom pain, which is pain that is perceived to originate from the digit or
segment of the digit that has been lost.
Having discussed the relevant anatomy and physiology and the ways the tissues of the digits are
likely to be injured subsequent to making contact with the blade of an operational table saw, it is
now possible to discuss the review team’s analysis of the 2017 NEISS table saw blade-contact
injuries and the extent to which the reported injuries fell into the above categories, as well as the
changes in injury diagnoses that were made.
3. Findings of Review Team’s Analysis of Table Saw Blade-Contact Injuries Treated in NEISS
System Emergency Rooms and Changes Made to Injury Diagnoses
Early on in the review of incidents, it became clear to the review team that, due to the complexity
and degree of the injuries that can occur, it was likely a difficult task for the NEISS coders to
assign an appropriate diagnosis code for certain table saw blade-contact injuries (the review team
faced the same difficulty). In large part, this is because NEISS coders are tasked with coding only
one injury diagnosis code for an incident. It is likely that this usually meant adopting the attending
physician’s primary diagnosis code, which in many cases can be very straightforward (providing
that the physician’s diagnosis is accurate). However, in other cases, it appears that the diagnosis
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
79
code may have been derived by other means, including choosing the injury that may have seemed
the worst.
In 55 incidents, the review team concluded that the diagnosis code was entirely incorrect, or
inaccurately conveyed the true extent of the injuries received. This easily can be illustrated with
a few examples. In an incident where a laceration from the table saw blade caused both a fracture
of bone and nerve damage, the coder would have been faced with having to choose from one of
three available diagnosis codes: laceration, fracture, or nerve damage. Only one code can be
assigned, but, in this case, none would do a particularly good job of conveying the true extent and
severity of the injuries. If in another incident, reported injuries from a table saw blade laceration
included a fracture and tendon damage, the coder would be forced to disregard the tendon damage
and choose from either laceration or fracture, as no diagnosis code exists for tendon damage.
Unfortunately, fracture would likely have been chosen, even if the fracture was so inconsequential
that no treatment for it was received, yet hours may have been required to repair the severed
tendons. Finally, if both tendon damage and injury to the vascular system are reported as a result
of a laceration from the table saw blade, the coder has no choice but to default to laceration injury,
because there is not a code for either tendon damage or vascular injury. This last example
highlights the deficiencies of the present system; such a laceration, which is obviously severe,
could end up in the same category with lacerations that are so minor that little or no blood was
shed.
Given the limitations of the available NEISS injury diagnosis codes, and the challenges presented
by injuries like those discussed above, the review team was forced to deliberate over these issues
and formulate a workable solution that would allow for a more comprehensive, accurate, and
repeatable way to characterize certain blade-contact injuries. Following a brief general overview
of the injuries reported in the 2017 NEISS incidents, the classification system that was ultimately
used by the review team will be discussed.
For all 161 of the 2017 completed table saw blade-contact IDIs that were analyzed, the injuries
were confined to the digit(s) and/or palm, or forearm, of one arm (i.e., either the left or right).
Specifically, 158 incidents involved either injuries to one or more digits (153), or to one or more
digits and the palm (5). The remaining three incidents involved injuries that were exclusively to
anatomical areas other than the digits; two incidents involved only the palm and one only the
forearm. The digits and palms involved in these incidents are illustrated in Figure 1; the one
forearm injury (of the right arm) is not illustrated. For both the left and right hand, the thumb and
index finger sustained the greatest number of digital injuries and the little finger the least.
Although injuries to the digits can occur anywhere along their length, the placement of the digits
on the workpiece and/or the course of movement one takes toward the blade means that the distal
portions of the digit are frequently involved. Of those incidents where handedness was known, a
slightly greater number of injuries involved the nondominant hand for both left-handed (60
percent) and right-handed (67 percent) individuals (See Table 1).
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

80
Figure 4. Left and right digits and palms involved in 160 of the 161 2017 NEISS
reported table saw blade-contact injuries; one injury, to the right forearm, is not
illustrated. Due to multiple injured digits or a combination of injured digit(s) and
a palm in many incidents, the total number of injuries depicted greatly exceeds the
number of incidents (i.e., 261 injured digits and palms were reported in 160
incidents).
Table 1. Hand dominance vs. side injured
Dominant Hand
Side Injured
Total
Left Right Unknown
Left 4 (40%) 6 (60%) 0 10
Right 85 (67%) 42 (33%) 0 127
Ambidextrous 9 0 0 9
Unknown 8 2 5 15
Total 106 50 5 161
During its review of the 161 IDIs, the review team determined in just over one third of the incidents
(55; 34 percent) that it was necessary to augment the injury diagnosis that was assigned to the
incidents by the NEISS coders (See Table 2). This was necessary either because the diagnosis
code was determined to be inappropriate or incorrect, or it failed to adequately capture the nature,
extent, or severity of the injuries and/or the necessary treatment (see below). Additionally, for 29
of the incidents (18 percent), the team determined that it was necessary to create a new injury
diagnosis, severe laceration, to better characterize those laceration injuries that were more severe
than simple lacerations, and for which no other injury diagnosis was entirely adequate. Most of
the severe lacerations involved injury to one or more of the deeper tissues. In a subset of these
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

81
severe lacerations, the wounds appear to have been just shy of an amputation injury; these were
often -coded by NEISS coders as amputations.
Table 2. Changes made to injury diagnoses
NEISS Reported
Injury Diagnosis
(Total)
Review Team Injury Diagnosis
Total
Laceration
Severe
Laceration
Amputation
Fracture Avulsion
Laceration (94) 71 19 2 2 94
Fracture (32) 10 6 5 11 32
Amputation (27) 3 3 19 2 27
Avulsion (7)
2 5 7
Nerve Damage (1) 1 1
Total 86 29 24 15 7 161
The justifications for the various changes to the injury diagnosis are as follows:
1. The NEISS diagnosis code was inappropriate or incorrect
From the evidence available to the review team, in 15 incidents the NEISS diagnosis code appeared
to be in error. In these cases, the diagnosis code was changed for one of three reasons:
a. In one incident, the correct diagnosis was provided in the NEISS narrative, but the
NEISS diagnosis code (mistakenly) provided a different injury diagnosis:
IDI 170921HEP9015 - the NEISS narrative states “…DX FINGERTIP AVULSION”;
the NEISS diagnosis code is Laceration; the review team diagnosis is Avulsion, based
on the evidence of an avulsion injury.
b. In seven incidents, the diagnosis code that was used was inappropriate. This occurred
most often when a laceration was mischaracterized as a partial amputation (i.e., coded
in NEISS as an amputation injury) when it really was a severe laceration or an
incomplete amputation, and/or was later surgically amputated.
Example: IDI 170228HEP9012 - the NEISS narrative states “…DX: PARTIAL
TRANSPHALANGEAL AMPUTATION, FINGER.”; the NEISS diagnosis code is
Amputation; the review team diagnosis is Fracture, based on multiple digits having
been fractured for which pins were placed, but none actually having been amputated.
Example: IDI 170331HEP9012 - the NEISS narrative states “…DX: AMPUTATION
L THUMB.”; the NEISS diagnosis code is Amputation; the review team diagnosis is
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
82
Severe Laceration, based on evidence that suggests that the severely injured digit was
surgically amputated.
c. In seven incidents, there was no evidence provided by the investigation to suggest that
the patient suffered an injury that was consistent with the NEISS diagnosis code.
Example: IDI 170427HEP9005 - the NEISS narrative states “…DX FINGERTIP
AMPUTATION…”; the NEISS diagnosis code is Amputation; the review team
diagnosis is Laceration, based on the described laceration injuries and the consumer’s
statement to the investigator that his digit “.. was NOT amputated. The injury was only
cosmetic.”
Example: IDI 170927HEP9011 - the NEISS narrative states “…NAIL AVULSION
LEFT 4
TH
FINGER…”, the NEISS diagnosis code is Avulsion; the review team
diagnosis is Laceration based on the evidence of only laceration injuries, and the
absence of any mention by the consumer of the loss of a nail.
2. NEISS diagnosis codes that failed to capture the complete extent or severity of the injuries
In 40 cases, the evidence available to the review team suggested that a different diagnosis code
would better capture the injuries that were received. In these cases, the diagnosis code was
changed for one of two reasons:
a. In 34 incidents, the evidence available to the review team suggested that a more severe
diagnosis would more accurately characterize the injuries and/or a different diagnosis
would more accurately characterize the complexity/cost of the necessary treatment.
Example: IDI 170202HEP9002 - the NEISS narrative states “…DX:..(R) HAND
WITH FLEXOR TENDON & DIGITAL NERVE DAMAGE.”; the NEISS diagnosis
code is Nerve Damage; the review team diagnosis is Severe Laceration, which captures
not only the nerve damage, but injuries to the flexor tendons, and nail plate (and
presumably also the blood vessels) that were treated with reconstructive surgery.
Example: IDI 170223HEP9008 - the NEISS narrative states “…DX: L THIRD
FINGER OPEN FX.”; the NEISS diagnosis code is Fracture; the review team diagnosis
is Severe Laceration, which better characterizes the scope and severity of injuries,
which included not only injury of the bone, but injuries to the nail bed and tendons that
required surgery and two nights in the hospital.
Example: IDI 170630HEP9006 - the NEISS narrative states “…FRACTURED
FINGER…”; the NEISS diagnosis code is Fracture; the review team diagnosis is
Amputation, based on evidence of the existence of an amputation (an injury that likely
included a fracture of bone).
Example: IDI 171108HEP9003 - the NEISS narrative states “…DX TENDON LAC
OF R HAND WITH OPEN FX”; the NEISS diagnosis code is Laceration; the review
team diagnosis is Severe Laceration, which better characterizes the scope and severity
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
83
of injuries, which included multiple fractures, laceration of tendons, and the need to
place multiple pins to reset bones.
b. In six incidents, the evidence available to the review team suggested that either a less
severe diagnosis would more accurately characterize the injuries and/or a different
diagnosis would more accurately characterize the complexity/cost of the necessary
treatment.
Example: IDI 170921HEP9006 - the NEISS narrative states “DX; OPEN FX…”; the
NEISS diagnosis code is Fracture; the review team diagnosis is Laceration, which
better characterizes the scope and severity of injuries, the treatment of which included
only stitches and bandaging, suggesting that the fracture was likely insignificant and
did not require any treatment to reset the bone.
The above changes resulted in the team avoiding usage of only one injury diagnosis code, Nerve
Damage, and adding another, Severe Laceration. Although the same number of injury diagnosis
codes was used by the NEISS coders and the review team, those used by the latter allowed a much
improved system for classifying the injuries.
For the most part, the injuries that were coded as Lacerations by the review team consisted of those
injuries that were simple lacerations; lacerations that did not affect deeper tissues. An exception
was for a subset of lacerations that also had open fractures that did not require any treatment; such
relatively insignificant fractures likely involved only the tuft of the terminal phalanx and it is
appropriate that they not be included with fractures requiring specialized reduction treatment to
reset the bone.
The addition of the Severe Laceration diagnosis allowed for a more accurate characterization of
those complex lacerations that affected one or more deeper tissues, including the digital nerves
and arteries, tendons, ligaments, and bone, and for which hospitalization and specialized treatment
was necessary, including microsurgical procedures, skin grafting, bone resetting, and other
surgeries. Use of this diagnosis alleviated the problem of there being no diagnosis code for some
injuries, including those to the vascular system, tendons, and ligaments. Some of the injuries that
were assigned the diagnosis of Severe Laceration were just short of being amputation injuries, and
some were so severe that, out of necessity, were surgically amputated by the physician who treated
the injuries.
Without the Severe Laceration diagnosis, a laceration that almost penetrated all the way through
the digit would have been relegated to either a laceration injury diagnosis or (usually) to a code
that only partially characterized the injuries (e.g., fracture); in such cases as the latter, although the
bone may be fractured, tendons cut, vascular system lacerated cleanly through, and nerve bundle
severed, it would have been characterized as only a fracture. This is misleading, as the treatment
and prognosis associated with an injury of this severity is dramatically different than a less severe
injury, such as a minor laceration with a tuft fracture; both may be coded as a fracture, but the
former may require hospitalization, surgical repair of nerves, blood vessels and tendons, and
setting of bones, whereas the latter may require only cleaning of the wound and bandaging. The
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
84
ability to classify it as a Severe Laceration is far more accurate and conveys the understanding that
one or more deeper tissues were likely to have been injured.
The Amputation diagnosis was reserved for only those injuries where the laceration resulted in the
complete transection of the digit, with separation of a part from the whole. In the present analysis,
all the amputations were partial amputations in that no digit in its entirety was amputated; instead,
only a portion of the digit was amputated. Incomplete amputations (i.e., those injuries where the
digit was not completely transected) were not considered amputations, and were, more
appropriately, categorized as Severe Lacerations. An exception to the use of this diagnosis code
was those amputations of the very tip of a digit, an injury that may heal spontaneously and require
no medical treatment beyond cleaning and bandaging of the wound — these injuries were
classified as laceration injuries.
Fracture as a diagnosis code is entirely appropriate and was used by the review team, even though
the bone is a deeper tissue. This is because fractures can occur in the absence of laceration injuries
to other deeper tissues. Use of this diagnosis code was limited to those fractures that were not
attended by injuries to other deeper tissues and were of significant severity that fusion of bone,
placement of pins, and/or other resetting procedures were required as part of the treatment.
The Avulsion diagnosis code was reserved for those incidents where the action of the blade
appeared to forcefully rip away a tissue or tissues from the digit. This is particularly appropriate
for when large sections of skin are avulsed, the nail plate is avulsed, and when the blade, via a
trenching action, removes a large volume of soft tissue.
Finally, it is important to at least touch on the additional complexity in the diagnostic picture that
occurs when multiple digits have been injured, as quite often not all of the digits may demonstrate
the same injury pattern. The review team applied similar logic in the assignment of an injury
diagnosis to these cases. For example, one or more digits may receive minor lacerations, whereas,
another may suffer an amputation at the distal interphalangeal joint. In this case, amputation may
be entirely appropriate as an injury diagnosis code. However, in another case, several digits may
suffer complex laceration injuries, whereas another may suffer a partial amputation very close to
the tip of the digit that requires no complex treatments. In this case, it is the severe laceration
injuries of the other digits that better captures the type and extent of the injuries received, the need
for hospitalization, and the complex and specialized surgeries and associated expense that are
necessary to treat these most serious injuries. Similarly, there may be multiple digits that have
been deeply lacerated, with significant loss of soft tissue, and likely damage to the nerves, and
another digit with a fracture of the tuft. In this case, the fracture is of little consequence — no
splinting, setting or other orthopedic manipulations take place and the wound is left open to heal
on its own; here a diagnosis of severe laceration is more appropriate.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
85
CONCLUSION:
In this memorandum, HS staff has provided a discussion of the anatomy and physiology of the
digits of the human hand and the degree to which they may be injured subsequent to contact with
a rotating table saw blade. Brief contact with the rapidly rotating saw blade of a table saw can
inflict wounds that range from a minor laceration of the epidermis to the far more complicated
amputation of a digit. Between these two extremes, the classification of injury type is more
complicated. In its analysis of the 2017 NEISS incidents involving table saw blade-contact
injuries, the review team was able to add clarity by the creation of a new diagnosis code, Severe
Laceration, and by following logical criteria for the use of the other injury diagnosis codes of
Laceration, Amputation, Fracture, and Avulsion, was able to classify all injuries in a
comprehensive, accurate, and repeatable manner.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

86
References
Agache P, Humbert P (2004) Measuring the skin. New York: Springer.
Alexander H, Miller DL (1979) Determining skin thickness with pulsed ultra sound. J Invest
Dermatol 72:17-9.
Baumann L (2007) Skin ageing and its treatment. J Pathol 211:241-251.
Burke FD (1984) Fingertip injuries and amputations. In: The Hand. (Birch R, Brooks D, eds), pp
210-225. Boston: Butterworths.
Doyle JR (2006) Hand and wrist. Philadelphia: Lippincott Williams & Wilkins.
Falabella AF, Falanga V (2004) Wound healing. In: The biology of the skin. Freinkel RK,
Woodley DT, eds. pp 281-293. New York: Parthenon Pub. Group.
Fassler PR (1996) Fingertip Injuries: Evaluation and Treatment. J Am Acad Orthop Surg 4:84-92.
Fornage BD, Deshayes JL (1986) Ultrasound of normal skin. J Clin Ultrasound 14:619-622.
Furlong R (1957) Injuries of the hand. London: J and A Churchill.
Gilchrest BA (1996) A review of skin ageing and its medical therapy. Br J Dermatol 135:867-
875.
Godfrey AM, Lister GD, Kleinert HE (1984) Replantation of the digits and hand. In: The Hand.
(Birch R, Brooks D, eds), pp 71-81. Boston: Butterworths.
Goldsmith L (1983) Biochemistry and physiology of the skin. New York: Oxford University Press.
Haake A, Scott GA, Holbrook KA (2004) Structure and function of the skin: overview of the
epidermis and dermis. In: The biology of the skin. Freinkel RK, Woodley DT, eds., pp 19-39.
New York: Parthenon Pub. Group.
Levit EK, Scher RK (2004) Basic science of the nail unit. In: The biology of the skin. Freinkel
RK, Woodley DT, eds., pp 101-108. New York: Parthenon Pub. Group.
Loda G (1999) Atlas of thumb and finger reconstruction. New York: Thieme.
Marble HC (1960) The hand: a manual and atlas for the general surgeon. Philadelphia: Saunders.
Mason S, Wardrope J, Turpin G, Rowlands A (2002) The psychological burden of injury: an 18
month prospective cohort study. Emerg Med 19:400-404.
Metze D, Luger T (2004) Nervous system in the skin. In: The biology of the skin. Freinkel RK,
Woodley DT, eds., pp 153-163. New York: Parthenon Pub. Group.
Montagna W, Carlisle K (1979) Structural changes in aging human skin. J Invest Dermatol 73:47-
53.
Moore TL, Lunt M, McManus B, Anderson ME, Herrick AL (2003) Seventeen-point dermal
ultrasound scoring system - a reliable measure of skin thickness in patients with systemic
sclerosis. Rheumatol 42:1559-1563.
Murai M, Lau H-K, Pereira BP, Pho RWH (1997) A cadaver study on volume and surface area of
the fingertip. J Hand Surg 22A:935-941.
Rayan G, Akelman E (2011) The hand: anatomy, examination, and diagnosis. Philadelphia:
Wolters Kluwer Health / Lippincott Williams & Wilkins.
Richard S, de Rigal J, de Lacharriere O, Berardesca E, Leveque J-L (1994) Noninvasive
measurement of the effect of lifetime exposure to the sun on the aged skin. Photodermatol
Photoimmunol Photomed 10:164-169.
de Rigal J, Escoffier C, Querleux B, Faivre B, Agache P, Leveque JL (1989) Assessment of aging
of the human skin by in vivo ultrasonic imaging. J Invest Dermatol 93:621-625.
Seidenari S, Pagnoni A, Di Nardo A, Giannetti A (1994) Echographic evaluation with image
analysis of normal skin: variations according to age and sex. Skin Pharmacol 7:201-209.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
87
Southwood WFW (1955) The thickness of the skin. Plast Reconstr Surg 15:423-429.
Tan CY, Statham B, Marks R, Payne PA (1982) Skin thickness measurement by pulsed ultrasound:
its reproducibility, validation and variability. Br J Dermatol 106:657-667.
Trott AT (2005) Wounds and lacerations: emergency care and closure. Philadelphia: Elsevier
Mosby.
Urbaniak JR (1979) Digit and hand replantation: current status. Neurosurgery 4:551-559.
Wittstadt RA (2005) Treatment options for distal tip amputations. In: The hand (Strickland JW,
Graham T, eds) pp 323-338. Philadelphia: Lippincott Williams and Wilkins.
Wood EJ, Bladon PT (1985) The human skin. Baltimore: E. Arnold.
Wysocki AB (1999) Skin anatomy, physiology, and pathophysiology. Nurs Clin North Am
34:777-797.
Zook EG (1990) Anatomy and physiology of the perionychium. Hand Clin 6:1-7.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
88
Tab C
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

UNITED STATES
CONSUMER PRODUCT SAFETY COMMISSION
4330 EAST WEST HIGHWAY
BETHESDA, MD 20814
Memorandum
89
Date: November 13, 2018
TO :
Caroleene Paul, Table Saw Project Manager
Division of Mechanical and Combustion Engineering
Directorate for Engineering Sciences
THROUGH :
Gregory B. Rodgers, Ph.D., Associate Executive Director,
Directorate for Economic Analysis
Robert Franklin, Senior Staff Coordinator,
Directorate for Economic Analysis
FROM :
Mark Bailey, Directorate for Economic Analysis
SUBJECT :
Table Saw Population Estimates for 2017
Background
The Directorate for Epidemiology conducted a special study of table saw blade-contact
injuries treated in U.S. hospital emergency departments (ED) during 2017 (Garland and Tu,
2018). The special study was conducted in support of ongoing rulemaking activities to develop a
mandatory standard to reduce blade-contact injuries and included IDIs of the table-saw injuries
that involved contact with the blade.
The purpose of this memorandum is to estimate the number of table saws in use in
2017,
52
and the proportion of table saws in use that were equipped with the modular blade guards
(MBG) required under the 7
th
edition of UL 987.
53
These estimates can then be compared to the
results of the 2017 special study of blade contact injuries to determine table saw injury rates and
evaluate the impact of MBGs on the risk of blade-contact injury.
This memorandum presents an overview of the methodology used to make the estimates,
and describes the results. Additionally, an appendix presents an analysis evaluating the
sensitivity of the risk of injury findings developed by the Directorate for Epidemiology to
possible variations in the estimated proportion of table saws equipped with the MBG systems.
52
The estimate of the number of table saws in use represents the number available for use; it does not represent a
measure of frequency of use.
53
The 7
th
edition of UL 987 was published in 2007. The effective date for the MBG requirements was January
2010, though some producers equipped their saws with the MBGs as early as 2007.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

90
Data Sources
Sales/Shipments
Aggregate annual table saw sales from 2002 through 2012 were provided by the Power
Tool Institute (PTI).
54,55
Annual sales for 2013 through 2017 were from a table saw market
research report published by Global Info Research (2018). (See Table 1). Global Info Research
also provided estimates for bench, contractor, cabinet, sliding, and other saws for the 2013 to
2017 time period, as shown in Table 1. In the absence of any information on market shares by
saw type prior to 2013, we assumed the proportional distribution of table saws by type prior to
2013 was equal to the 5-year average for the 2013-2017 time period. Based on the Global Info
Research data, the 5-year average for bench, contractor, cabinet, sliding, and other saws
accounted for 79 percent, 10 percent, 6 percent, 3 percent, and 2 percent of sales respectively.
Table saw sales, by type, are shown in Table 1. For purposes of this analysis, and consistent
with procedures used in the preliminary regulatory analysis for the table saw notice of proposed
rulemaking (NPR) (Zamula, Rodgers, and Bailey, 2016), we combined sliding saws with cabinet
saws and the saws categorized as “other” (which were probably hybrid saws) with contractor
saws.
Table 1. Annual Table Saw Sales by Type (Thousands)
Year
Total
Bench Saws
Contractor Saws
Cabinet Saws
Sliding
Others
2002
725
573
73
44
22
15
2003
750
593
75
45
23
15
2004
775
612
78
47
23
16
2005
800
632
80
48
24
16
2006
825
652
83
50
25
17
2007
825
652
83
50
25
17
2008
650
514
65
39
20
13
2009
589
465
59
35
18
12
2010
429
339
43
26
13
9
2011
600
474
60
36
18
12
2012
625
494
63
38
19
13
2013
609
477
65
37
17
13
2014
625
494
63
37
18
13
2015
646
514
65
36
18
13
2016
625
496
63
36
17
13
2017
651
517
65
38
17
14
Source: Power Tool Institute, Global Info Research
54
PTI annual estimates were reported on the PTI website or provided to the U.S. Consumer Product Safety
Commission (CPSC) by means of personal communication with staff. For the years 2006 and 2007 PTI provided a
range for the sales estimate rather than an exact number. We used a simple mean of that range for these two years.
This data was used in the regulatory analysis contained in the CPSC’s 2017 notice of proposed rulemaking (NPR).
See Table 4 Tab C of Commission Briefing package “Proposed Rule: Safety Standard Addressing Blade-Contact
Injuries on Table Saws.”
55
PTI provided total estimated sales for all table saws; PTI did not provide estimates by table saw type.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
91
Expected Product Life by Saw Type
The preliminary regulatory analysis for the 2017 NPR used an expected product life of 10
years for bench saws, 17 years for contractor saws (including hybrids), and 24 years for cabinet
saws (including sliding). These estimates were based on information provided by PTI in a
meeting with Commissioner Adler on March 2, 2011. However, in PTI’s comment on the NPR,
PTI asserted that bench saws have an average expected product life of about 7.5 years, rather
than 10 years. Consequently, in estimating the population of table saws available for use, we
used a 7.5 year expected product life for bench saws, as submitted by PTI in its formal comment
on the proposed rule.
Sales of Saws Equipped with MBGs
PTI also provided sales estimates on the number of table saws equipped with the modular
blade guard systems required under the 7
th
edition of UL 987. These estimates were published by
PTI on their webpage PTI Facts at a Glance, which is updated regularly. PTI estimated that:
• “Since 2007 [through 2010], PTI members have introduced over 800,000 saws with the
newly designed guards which meet the requirements of UL 987 safety standard.”(PTI,
2011);
• “From 2007 through the end of 2014, PTI members have introduced over 2.6 million
saws with the newly designed guards which meet the requirements of the newly revised
UL 987 safety standard” (PTI, 2016); and finally,
• “From 2007 through the end of 2017, PTI members have introduced over 4.3 million
saws in the U.S. with the newly designed modular guarding systems, including a riving
knife, which meet the relevant requirements of the 7
th
and 8
th
editions of UL 987 and UL
62841-3-1 safety standards” (PTI, 2018).
Based on (1) PTI estimates of saws equipped with MBGs, (2) the sales estimates
presented in Table 1, (3) the PTI estimate that their members account for approximately 80
percent of the sales of all table saws in the U.S. (PTI, 2012), and (4) the assumption that non-PTI
members equipped their saws at roughly the same rate as PTI members, we project that saws
equipped with the MBG systems accounted for about 30 percent of sales from 2007 through
2010, 90 percent of the saws sold from 2011 through 2014, and 100 percent of the saws sold
from 2015 through 2017.
Methodology and Results
Estimating the Table Saw Population in Use for 2017
The annual number of table saws in use was estimated with the CPSC’s Product
Population Model (PPM), a statistical model that projects the number of products in use given
estimates of annual product sales and information on product failure rates over time (Gordon and
Lahr, 1980). For this analysis, we estimated the population of each type of table saw in 2017,
based on the annual sales for each type (Table 1) in combination with information on the
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
92
expected product life provided by PTI. The failure rate for each type of saw was assumed to
follow a gamma distribution (with a shape parameter of 3), which is a commonly used
distribution for modeling product failure rates. Totals for 2017 were then aggregated as the
summation of the estimated population for each saw type. Based on this analysis, there were an
estimated 6.86 million table saws in use in 2017.
Estimating the Population of Saws in Use Equipped with the MBG system in 2017
The annual number of table saws in use equipped with the MBG system was estimated
using the share of saw sales estimated for the years 2007 through 2017 and determining what
proportion of the saws equipped with MBGs remained in use in 2017. Based on this analysis, we
estimate that 3.94 million, or 57.4 percent, of the table saws in use in 2017 were equipped with
MBGs.
Attachment: Sensitivity Analysis
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

93
Works Cited
Garland, Sarah, Tu, Yongling , 2018. Table Saw Blade-Contact Injuries Special Study Report,
2017. U.S. Consumer Product Safety Commission, November 2018.
Global Info Research, 2018. Global Table Saws Market by Manufacturers Countries Type and
Application Forecast to 2023. Global Info Research, Hong Kong, June 2018.
Gordon, B.B., Lahr M.L. 1980 Product Life Model Feasibility and Developmental Study.
Contract CPSC-C-79-009, Task 6, Subtasks 6.01-6.06. Columbus, OH. Battelle, July 1980.
PTI, 2011. Table Saw Facts at-a-Glance. Accessed June 15, 2011, at:
http://www.powertoolinstitute.com/pti-pages/it-table-saw-facts.asp
PTI, 2012. Comment by Susan M. Young for the Power Tool Institute, Inc., on “U.S. Consumer
Product Commission [Docket No. CPSC-2011-0074] Table saw blade contact injuries: Advance
notice of proposed rulemaking,” (March 16, 2012). (Comment CPSC-2011-0074-1081, available
at: regulations.gov)
PTI, 2016. Table Saw Facts at-a-Glance. Accessed June 20, 2016, at:
http://www.powertoolinstitute.com/pti-pages/it-table-saw-facts.asp
PTI, 2017. Comment by Susan M. Young for the Power Tool Institute, Inc., on “U.S. Consumer
Product Commission [Docket No. CPSC-2011-0074] Safety Standard Addressing Blade-Contact
Injuries on Table Saws; Notice of Proposed Rulemaking” (July 26, 2017). (Comment CPSC-
2011-0074-1288, available at: regulations.gov)
PTI, 2018. Table Saw Facts at-a-Glance. Accessed September 19, 2018, at:
http://www.powertoolinstitute.com/pti-pages/it-table-saw-facts.asp
Zamula, W. William, Rodgers B. Gregory, and Bailey, Mark, 2016. Preliminary Regulatory
Analysis of the Draft Proposed Rule for Table Saws. U.S. Consumer Product Safety
Commission, December 2016.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
94
Appendix: Sensitivity of relative risk estimates to variations in exposure estimates
Using information from the 2017 special study of table saw blade-contact injuries treated
in U.S. hospital emergency departments (Garland and Tu, 2018), in combination with estimates
of the number of table saws in use and estimates of the proportion of tables saws in use that were
equipped with the modular blade guards (MBG required by the 7
th
edition of UL 987, the
Directorate for Epidemiology estimated about 6,075 ED injuries per million table saws equipped
with a traditional (pre-modular) blade guard system, compared to about 819 ED injuries per
million table saws equipped with the MBG system. This yielded a relative risk of about 7.4 (i.e.,
6,075 injuries per million saws with traditional blade guards ÷ 819 injuries per million saws with
MBGs), suggesting that the MBSs may have reduced the blade-contact injury risk by about 86.5
percent (i.e., (6,075 − 819) ÷ 6,075).
This appendix describes the results of an analysis designed to evaluate the sensitivity of
the relative risk estimate to variations in the possible distribution of injuries where the presence
of an MBG on the original equipment could not be determined, variations in the estimated
number of table saws in use, and variations in the estimated proportion of saws in use that were
equipped with the MBGs.
The estimate of table saws in use in 2017 and the proportion of those in use that were
equipped with the MBGs required under the 7
th
edition of UL 987 (described in the body of this
memorandum), were based on:
• annual total table saw sales estimates provided by PTI for 2002 through 2012;
• annual total sales estimates from Global Info Research (2018) for 2013 through
2017;
• table saw sales, by type, from Global Info Research (2018) for 2013 through
2017;
• an assumption that the percentage market share of sales by saw type for saws sold
prior to 2013 was the same as the average market share during the 2013-2017
time period;
• estimates, based on information provided by PTI, that about 30 percent of table
saws sold from 2007 through 2010 were equipped with the MBG systems, 90
percent of tables saw sold from 2011 through 2014 were equipped with MBGs,
and 100 percent of saws sold from 2015 through 2017 were equipped with
MBGs; and
• PTI estimates of the expected average product life of bench, contractor, and
cabinet saws, which were 7.5 years, 17 years, and 24 years, respectively.
Based on these estimates, the Directorate for Economic Analysis projected an estimated
6.86 million table saws in use in 2017, with about 57.4 percent equipped with the MBGs.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

95
First Sensitivity Evaluation
To conduct the initial sensitivity evaluation, we separated the ED injury estimates into
three categories: those not equipped with MBGs,
56
those equipped with MBGs (i.e., those
conforming to the voluntary standard’s MBG requirements), and those injuries for which it could
not be determined whether the saws had been equipped with MBGs (i.e., the “unknowns”). We
then evaluated how the distribution of the unknowns could have affected the relative risk
estimate, given the estimate of table saws in use and the proportion equipped with MBGs. More
specifically, we looked at three alternative assumptions: (a) that the injuries involving blade
guards categorized as unknown were distributed proportionally to the knowns; (b) that all of the
“unknowns” involved saws not equipped with MBGs, and (c) that all of the “unknowns”
involved saws equipped with MBGs. Note that while both alternatives (b) and (c) are unlikely,
they nevertheless provide the outer bounds for alternative (a).
The results of this analysis are presented in Part 1 of Table 2, which appears later in this
appendix. The base injury rate for our analysis assumed that the unknowns (5,200 ED injuries)
were distributed proportionally to the knowns (column 3). This alternative resulted in a relative
risk of 7.63 (i.e., 7,707 injuries per million saws not equipped with MBGs ÷ 1,010 injuries per
million equipped with MBGs), suggesting that MBGs reduced the risk by 86.9 percent (i.e.,
(7,707 − 1,010) ÷ 7,707).
57
This relative risk was bounded by a relative risk estimate of 9.82
under the assumption that all of the 5,200 unknowns had no MBGs (column 4) suggesting a risk
reduction 89.9 percent, and a relative risk estimate of 2.91 under the assumption that all the
unknowns had been equipped with the MBGs (column 5) and suggesting a risk reduction of 65.6
percent.
Second Sensitivity Evaluation
Because the preliminary regulatory analysis assumed an expected product life of 10 years
for bench saws (Zamula, Rodgers, and Bailey, 2016), rather than the 7.5-year estimate currently
recommended by PTI,
58
we also conducted a sensitivity analysis based on the 10-year product
life assumption to determine how the results would have varied given the assumptions used in
the preliminary regulatory analysis contained in the 2017 notice of proposed rulemaking (NPR).
Given this longer hypothesized product life for bench saws, we projected an estimated
8.20 million table saws in use in 2017, with 51.9 percent having been equipped with the MBGs,
compared to the 6.86 million and 57.4 percent estimates for the 7.5-year product life assumption.
Using these revised estimates with a 10-year bench saw expect life, we again evaluated how the
distribution of the injury unknowns could have affected the relative risk estimate, as we did in
the first sensitivity evaluation. The results of this second analysis are presented in Part 2 of
Table 2. The base injury rate for our sensitivity analysis assumed that the unknowns (5,200 ED
56
From Table 16 of Garland and Tu (2018), these included the 102 injury cases involving tables saws determined to
have been originally equipped with “traditional” pre-modular blade guards and the single injury case which was
categorized as not applicable or none because it was believed to have been too old to have been originally equipped
with any blade guard at all, let alone the MBG.
57
Because the unknowns are distributed proportionally to the knowns in column (3), the relative risks are
necessarily identical to those calculated in column (2).
58
The expected product life for contractor and cabinet saws in the preliminary regulatory analysis were 17 and 24
years, respectively, which were consistent with the current PTI recommendations.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

96
injuries) were distributed proportionally to the knowns (column 3). This alternative resulted in a
relative risk of 6.11, suggesting that the MBG system would have reduced the injury risk by
about 83.6 percent. This relative risk was bounded by a relative risk estimate of 7.87, suggesting
a risk reduction 87.3 percent (column 4), and a relative risk estimate of 2.33, suggesting a risk
reduction of 57.1 percent (column 5).
Third Sensitivity Evaluation
In 2007, UL published the seventh edition of UL 987, which expanded the table saw
blade guard requirements to include the MBG design developed by the joint venture of the
leading table saw manufacturers. The effective date for the MBG requirements was January
2010. As described above, PTI estimated that about 30 percent of table saws sold during 2007
through 2010 were equipped with the MBG. Because three of these four years were prior to the
January 2010 effective date, we evaluated the impact of an assumption that no table saws during
the entire 2007 through 2010 time period were equipped with the MBGs, contrary to PTI
estimates.
These results are presented in Part 3 of Table 2. We again evaluated how the distribution
of the injury unknowns could have affected the relative risk estimate, as we did in the first and
second sensitivity evaluations. The base injury rate for this sensitivity analysis assumed that the
unknowns (5,200 ED injuries) were distributed proportionally to the knowns (column 3). This
alternative resulted in a relative risk 6.29, suggesting that the MBG system would have reduced
the injury risk by about 84.1 percent. This relative risk was bounded by a relative risk estimate
of 8.10, suggesting a risk reduction 87.7 percent (column 4), and a relative risk estimate of 2.40,
suggesting a risk reduction of 58.3 percent (column 5).
Fourth Sensitivity Evaluation
We conducted a fourth sensitivity evaluation based on relative risks derived from the
approximate 95 percent confidence interval (CI) for injury rates presented by the Directorate for
Epidemiology. Based on Garland and Tu (2018), an approximate 95 percent CI for table saws
not equipped with the MGS ranged from 5,753 to 6,399 injuries per million, and the approximate
95 percent CI for table saws with modular blades ranged from 748 to 890 injuries per million.
Using these estimates, relative risks could have ranged from 8.55 (6,399 ÷ 748) to 6.46 (5,753 ÷
890). These two relative risks suggest an injury rate reduction associated with the MBG of 88.3
percent and 84.5 percent, respectively.
Fifth Sensitivity Evaluation
By basing estimates of relative risk on the numbers of saws in use, the analyses above
implicitly assumed that table saw usage was proportional to the numbers of table saws in use,
and that the average usage time per table saw for those equipped with MBGs was about the same
as for saws not equipped with MBGs. However, if the average usage time for saws not equipped
with the MBGs were greater than the average usage time for saws equipped with MBGs, then the
relative risk associated with the saws not equipped with the MBGs would have been
overestimated. While we have no empirical basis for assuming that the average usage time per
table saw for those equipped with MBGs was about the same as for saws not equipped with
MBGs, we conducted a sensitivity evaluation to determine how sensitive our results would have
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

97
been to such an assumption. If saws not equipped with MBGs were, on average, used twice as
much as those with MBGs, then relative risks could be approximated in Part 1 by doubling the
estimate of table saws in use from 2.92 million to 5.84 million. The estimate of relative risk
from part 1, column 3, would therefore decrease from 7.63 to 3.82 (i.e., [22,519 injuries ÷ (2 ×
2.92 million table saws in use)] ÷ 1,010 injuries/million saws), suggesting a risk reduction of
about 73.8 percent relative to the risk on saws with MBGs.
59
’
60
Similarly, this risk reduction
would be bounded by a relative risk of 4.91 (part 1, column 4), suggesting a risk reduction of
about 79.6 percent, to a relative risk of 1.45 (part 1, column 5), suggesting a risk reduction of
31.2 percent.
Summary of Results
Given the available data, the results of this sensitivity analysis appear to be quite strong
with respect to the estimated numbers of table saws in use. The sensitivity analysis suggests that
the risk reduction associated with the MBG system is largely driven by the relatively small
proportion of injuries (about 15 percent) involving saws equipped with the MBGs, and not the
various assumptions applied to obtain estimates of table saws in use. Substantial reductions in
the estimate of the proportion of table saws equipped with the MBG system, as required by the
current voluntary standard, would be needed to alter the statistically significant difference in the
injury risks between non-modular and modular blade guard saws reported in table 12 of Garland
and Tu (2018).
59
Based on the Part 1, column (3) assumptions, the usage of saws without MBGs would have to increase by a factor
of about 7.6 for the risks on saws without MBGs to equal the risk on saws with MBGs (i.e., (i.e., [22,519
injuries/million saws ÷ (7.6 × 2.92 table saws in use)]÷ 1,010 injuries/million saws = 1)
60
It is also possible that table saws equipped with MBGs are used, on average, more than saws not so equipped.
However, because this would result in an even greater relative risk on saws without MBG, we have not explicitly
included it in this analysis.
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)

98
Table 2: Estimated Risks and Relative Risks associated with table saws modular blade guard (MBG) systems, 2017
(1) (2) (3)* (4) (5)
Table Saws
Original distribution Unknowns distributed Unknowns assumed to
Unknowns assumed to
in Use of ED injuries proportionately involve non-modular BG involve modular BG
(in millions) ED Injuries Risk** ED Injuries Risk** ED Injuries Risk**
ED Injuries
Risk**
Part 1 Total Table Saws*** 6.86 26,500 3,861
Equipped with:
No MBG 2.92 18,100 6,195 22,519 7,707 23,300 7,974 18,100 6,195
MBG 3.94 3,200 812 3,981 1,010 3,200 812 8,400 2,131
Unknown 5,200 NA
Relative Risk 7.63 7.63 9.82 2.91
Injury Rate Reduction 86.9% 86.9% 89.8% 65.6%
Table Saws
(in millions) ED Injuries Risk** ED Injuries Risk** ED Injuries Risk**
ED Injuries
Risk**
Part 2 Total Tables Saws**** 8.20 26,500 3,231
Equipped with:
No MBG 3.94 18,100 4,591 22,519 5,712 23,300 5,910 18,100 4,591
MBG 4.26 3,200 751 3,981 934 3,200 751 8,400 1,972
Unknown 5,200
Relative Risk 6.11 6.11 7.87 2.33
Injury Rate Reduction 83.6% 83.6% 87.3% 57.1%
Table Saws
(in millions) ED Injuries Risk** ED Injuries Risk** ED Injuries Risk**
ED Injuries
Risk**
Part 3 Total Table Saws***** 6.86 26,500 3,861
Equipped with:
No MBG 3.25 18,100 5,572 22,519 6,932 23,300 7,173 18,100 5,572
MBG 3.61 3,200 885 3,981 1,101 3,200 885 8,400 2,324
Unknown 5200 NA
Relative Risk 6.29 6.29 8.10 2.40
Injury Rate Reduction 84.1% 84.1% 87.7% 58.3%
* Because the unknowns are distributed proportionally to the knowns, the relative risks in column (3) are identical to those calculated in column (2).
**ED Injuries per million table saws in use
*** Assumes an expected product life of 7.5 years for bench saws, 17 years for contractor saws, and 24 years for cabinet saws
**** Assumes an expected product life of 10 years for bench saws, 17 years for contractor saws, and 24 years for cabinet saws
***** Assumes no table saws were equipped with MGBs during 2007-2010
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
99
THIS DOCUMENT HAS NOT BEEN REVIEWED
OR ACCEPTED BY THE COMMISSION.
CLEARED FOR PUBLIC RELEASE
UNDER CPSA 6(b)(1)
