
Policies to Achieve
Near-Universal Health
Insurance Coverage
CONGRESS OF THE UNITED STATES
CONGRESSIONAL BUDGET OFFICE
OCTOBER 2020
© Monster Ztudio/Shutterstock.com

At a Glance
In this report, the Congressional Budget Oce examines policy approaches that could achieve near-universal
health insurance coverage using some form of automatic coverage through a default plan. As dened by CBO,
a proposal would achieve near-universal coverage if close to 99percent of citizens and noncitizens who are
lawfully present in this country were insured either by enrolling in a comprehensive major medical plan or
government program or by receiving automatic coverage through a default plan.
Components of Proposals at Would Achieve Near-Universal Coverage
Policy approaches that achieved near-universal coverage would have two primary features:
•
At a minimum, if they required premiums, those premiums would be subsidized for low- and moderate-
income people, and
•
ey would include a mandatory component that would not allow people to forgo coverage or that would
provide such coverage automatically.
e mandatory component could take the form of a large and strongly enforced individual mandate pen-
alty—which would induce people to enroll in a plan on their own by penalizing them if they did not—or a
default plan that would provide automatic coverage for people who did not purchase a health insurance plan
on their own during periods in which they did not have an alternative source of insurance. Because lawmak-
ers recently eliminated the individual mandate penalty that was established by the Aordable Care Act, this
report focuses on approaches that could achieve near-universal coverage by using premium subsidies and
dierent forms of automatic coverage through a default plan.
Policy Approaches
CBO organized existing proposals into four general approaches, ranging from one that would retain existing
sources of coverage to one that would almost entirely replace the current system with a government-run program.
All four approaches would provide automatic coverage to people who did not enroll in a plan on their own.
•
Two approaches would fully subsidize coverage for lower-income people and partially subsidize coverage
for middle-income and some higher-income people while retaining employment-based coverage.
Financing would come, in part, from broad-based tax revenues that were not linked to health insurance
coverage. Financing also would come from higher taxes on those uninsured people who were covered by
the default plan and whose premiums were not fully subsidized; those taxes would be equivalent to their
share of the premium. Collecting such taxes from uninsured people would pose challenges.
•
Two approaches would fully subsidize coverage for people at all income levels. Financing would come
entirely from broad-based tax revenues, and people who did not enroll in a health insurance plan would
not owe additional taxes.
Under some approaches, the default plan would be privately managed. Under others, it would be a public
plan, operated by the federal government.
e approaches that CBO examined would require varying amounts of government spending to cover the
same number of people. ey would all require additional federal receipts to achieve decit neutrality.
www.cbo.gov/publication/56620

Contents
Summary 1
Essential Components of Near-Universal Health Insurance Coverage and an
Overview of the Approaches at CBO Analyzed 1
How Subsidies Would Aect Default Coverage Under Dierent Approaches 2
Challenges Associated With Implementing Automatic Coverage rough a Default Plan 3
Policy Approaches at Could Achieve Near-Universal Coverage by Using a Default Plan 3
Background and Scope of the Report 8
Denition of Health Insurance Status and Coverage 8
Sources of Coverage and Uninsured People Under Current Law 9
Legislative Proposals to Incrementally Expand Access to Coverage and Reduce
Out-of-Pocket Premiums 11
Strategies to Achieve Near-Universal Coverage 11
Scope of the Report 13
Automatic Coverage Through a Default Plan for People Without an Alternative
Source of Health Insurance: Design Considerations and Challenges 13
Enrollment in a Default Plan and Use of Health Care Under at Plan 13
Key Design Choices Associated With Default Coverage 15
Key Challenges of Implementing Default Coverage 16
Policy Approaches 20
Approach 1: Partially Subsidized Default Coverage at Operates in Tandem With
Current Sources of Coverage 20
BOX 1. INTRODUCING DEFAULT COVERAGE WHILE MAINTAINING AN EMPLOYER
FIREWALL: IMPLICATIONS AND CHALLENGES 22
Approach 2: Partially Subsidized Default Coverage rough a Large Public
Program at Replaces Medicaid, CHIP, and the Nongroup Market and Retains
Employment-Based Coverage 26
Approach 3: Premium Subsidies for All People and Default Coverage rough a Fully Subsidized Plan 29
Approach 4: A Single-Payer System 31
List of Tables and Figures 33
About This Document 34

Notes
As referred to in this report, the Aordable Care Act comprises the Patient Protection and
Aordable Care Act (Public Law111-148), the health care provisions of the Health Care
and Education Reconciliation Act of 2010(P.L.111-152), and the eects of subsequent
judicial decisions, statutory changes, and administrative actions.

Policies to Achieve Near-Universal
Health Insurance Coverage
Summary
In this report, the Congressional Budget Oce exam-
ines policy approaches that could achieve near-universal
health insurance coverage. Such approaches would pro-
vide nearly all people in the United States with nancial
protection against high-cost medical events, increase
overall access to health care, and decrease the costs that
providers incur when they provide medical services to
uninsured people. e approaches also would increase
federal subsidies for health care.
As dened by CBO, a proposal would achieve near-
universal coverage if close to 99percent of citizens and
noncitizens who are lawfully present in this country
were insured either by enrolling in comprehensive major
medical coverage or by receiving automatic coverage
through a default plan. Attaining such coverage would be
challenging, however. CBO is not aware of any existing
proposals—legislative or otherwise—that would achieve
complete (that is, 100percent) universal coverage
because they all would require some demonstration of
eligibility (such as meeting criteria related to citizenship
or residency) that some eligible people would not comply
with for various reasons.
Essential Components of Near-Universal Health
Insurance Coverage and an Overview of the
Approaches That CBO Analyzed
In CBO’s view, to attain near-universal coverage, a policy
would need to provide premium subsidies for low- and
moderate-income people and include a mandatory com-
ponent that would not allow people to forgo coverage.
Subsidizing premiums for low- and moderate-income
people would be essential because paying the full cost
of comprehensive major medical coverage out of pocket
would typically be prohibitive. A mandatory compo-
nent would be essential because some people would still
choose not to purchase insurance even if they had the
means to do so. e mandatory component could take
the form of a requirement that people purchase health
insurance (sometimes known as an individual mandate),
which would be strongly enforced with a large penalty,
or it could provide automatic coverage through a default
plan for people who did not purchase a health insurance
plan of their choice.
Because the Congress recently eliminated the individual
mandate penalty that was established by the Aordable
Care Act (ACA), CBO did not focus on approaches that
would achieve near-universal coverage using such a man-
date. Instead, CBO focused on approaches that would
attain near-universal coverage by using premium subsi-
dies and dierent forms of automatic coverage through
a default plan. (CBO uses the term “default plan” to
describe a plan that would provide automatic coverage
to people during periods in which they did not have an
alternative source of insurance; eligible people could use
it to receive medical care at any time.)
Under an individual mandate, a penalty is levied on peo-
ple who do not enroll in a plan. Although those people
are required to make a payment, they do not have any
coverage. If the penalty was large and strongly enforced,
then nearly all people would choose to purchase insur-
ance rather than pay the penalty. By contrast, with
automatic coverage through a default plan, the govern-
ment provides or procures insurance for people who do
not purchase it on their own and nances the cost of
that coverage through the tax system. Financing could
come entirely from broad-based revenues if the default
plan was fully subsidized, or it could come, in part, from
premium-equivalent tax payments levied on people who
did not purchase a plan on their own.
In this report, CBO describes the key features—specif-
ically, the enrollment process, premiums, cost sharing
and benets, and the role of private insurance, public
programs, and employment-based insurance—of four

2 Policies to Achieve NeAr-UNiversAl heAlth iNsUrANce coverAge october 2020
general approaches that could achieve near-universal
coverage by using premium subsidies and dierent forms
of automatic coverage through a default plan. ose
approaches are as follows:
•
Approach 1. A multipayer system that retains existing
sources of coverage while expanding eligibility for
premium subsidies and providing partially subsidized
default coverage through a private plan or a new
public option.
1
•
Approach 2. A multipayer system that retains
employment-based coverage and replaces the current
nongroup market and the acute care portions of
Medicaid and the Children’s Health Insurance
Program (CHIP) with a new public program that
allows people to choose between partially subsidized
private plans and a publicly administered plan that
provides default coverage.
•
Approach 3. A multipayer system that provides full
subsidies for all people to purchase a private plan
of their choice, with a default plan that provides
automatic coverage to people who do not enroll in a
plan on their own.
•
Approach 4. A single-payer system that acts as a
default plan for all people.
ose four general approaches encompass all of the
detailed proposals that CBO has identied as potentially
achieving near-universal coverage without the use of a
large and strongly enforced individual mandate penalty.
Although the four approaches described in this report
have the potential to achieve near-universal coverage,
CBO has not analyzed specic proposals in detail.
is report focuses on people under the age of 65; the
Medicare program could continue to provide coverage to
people age 65or older under all of the approaches except
for the one that would adopt a single-payer system. e
report does not discuss eects on national health expen-
ditures (NHE), which might increase or decrease under
dierent approaches depending on the details of the pro-
posal. Approaches that lowered out-of-pocket costs would
increase NHE by encouraging greater use of health care,
but that increase could be oset by other features, such as
lower provider prices, that would result in lower NHE.
1. A multipayer health care system is one in which more than one
insurer provides health insurance coverage.
e approaches CBO examined would require varying
amounts of government spending to cover the same
number of people, but they would all require at least
some additional federal receipts to achieve decit neutral-
ity. Whether the adopted approach is decit-neutral is a
choice that policymakers would need to make. Much of
the new federal costs would stem from the additional tax
credits or other subsidies that would be made available to
people. Some of those subsidies would reduce or elimi-
nate the out-of-pocket premiums of people who would
have been uninsured under the current system, and some
would go to people who would have had coverage any-
way under the current system. Reallocating existing fed-
eral subsidies for health care (such as uncompensated care
payments and grants to community health centers) and
for other sources of coverage (such as the tax exclusion
for employment-based coverage) would not be sucient
to entirely nance the additional federal costs that would
be incurred under the four approaches. A complete
discussion of how the subsidies for coverage expansions
would be nanced is outside the scope of the report.
How Subsidies Would Aect Default Coverage
Under Dierent Approaches
All four of the approaches described in this report would
provide automatic coverage through a default plan, but
the role of default coverage would vary under each of the
approaches. Specically:
•
e rst two approaches would fully subsidize default
coverage for lower-income people and partially
subsidize coverage for middle-income and some
higher-income people. Under those approaches, the
government would collect premium-equivalent tax
payments from middle- and higher-income people
who did not have an alternative source of insurance.
Levying taxes on those people would be the
equivalent of charging mandatory premiums for the
default plan. To maintain incentives to enroll in other
sources of coverage, the amount of the tax associated
with default coverage would be made equivalent to
the net premium the person would pay to actively
enroll in a plan that provided similar benets.
•
e last two approaches would fully subsidize
default coverage for people at all income levels,
and no premium-equivalent tax payments would
be collected. ose approaches could be nanced
through broad-based tax revenues that are not linked
to people’s health insurance coverage.

3october 2020 Policies to Achieve NeAr-UNiversAl heAlth iNsUrANce coverAge
Challenges Associated With Implementing
Automatic Coverage Through a Default Plan
Providing automatic coverage through a default plan to
achieve near-universal coverage would present several
challenges, particularly if the plan was only partially
subsidized. Additional challenges would arise if the
default plan was part of a risk-adjustment system that
shared the cost of insuring a group of enrollees across
all plans, as the current nongroup market does. (e
nongroup market is a private health insurance market
that enables individuals and families who are not eligible
for coverage through public programs or who do not
have employment-based insurance to purchase a private
health insurance policy.) ere also would be challenges
associated with informing people about their eligibility
for default coverage and its associated benets, particu-
larly the plan’s provider network.
Collecting premium-equivalent tax payments when
default coverage was partially subsidized would require
verifying the coverage status of all tax lers, which would
be administratively complex. Although uninsured people
would gain coverage through a default plan, many people
might be surprised by the new premium-equivalent tax
that would be required to nance their coverage if taxes
were collected many months after the period during
which they were uninsured (unlike a premium, which is
collected at the time a person enrolls in health insurance).
at tax obligation could total thousands or even tens of
thousands of dollars, particularly for the highest-income
families who would not qualify for any subsidies.
Additional complexities would arise if the default plan
shared the cost of insuring more or less costly people
with other plans through the same risk-adjustment
system. Determining the appropriate risk-adjustment
payments to plans (which adjust their premiums for the
cost of their enrollees) would be challenging because it
would require the government to determine the num-
ber of people covered by the default plan and the cost
to insure them relative to the cost of people covered by
other plans in the risk-adjustment system.
e government also would need to inform people about
their eligibility for default coverage and the benets asso-
ciated with that coverage. An outreach campaign could
educate people about their eligibility for the default plan
and its associated benets, but it would be dicult to
fully inform all people. If some providers did not par-
ticipate in the default plan’s network, informing people
about which providers did participate would present par-
ticular challenges. Some people might seek care without
knowing whether a provider participated in the default
plan’s network and might be unexpectedly billed large
amounts for their care if they received treatment from a
nonparticipating provider.
Policy Approaches That Could Achieve
Near-Universal Coverage by Using a Default Plan
CBO analyzed four approaches that have the potential to
achieve near-universal coverage by using both premium
subsidies and a form of default coverage. Each approach
involves a general strategy for covering all people in a
dened population, and the approaches have multiple
variants and design choices, such as how much to sub-
sidize premiums and the degree of cost sharing. (For a
summary of approaches to achieve near-universal health
insurance coverage through a default plan, see Table 1.
For key features of approaches to achieve near-universal
health insurance coverage through a default plan as com-
pared with current law, see Table 2.)
Each successive approach would require more signicant
changes to the current system and, in general, would
be more costly to the federal government. Approaches
that involved more incremental changes to the current
system—specically, Approaches 1 and 2—would entail
fewer transition costs and changes to existing sources of
coverage, but they would impose new tax obligations
on some people who did not enroll in a plan, and the
resulting system would be more complex than under
the other approaches. Approaches that involved more
signicant changes to the current system—Approaches 3
and 4—would require larger transition costs and changes
to sources of coverage, but enrolling people in coverage
would be simpler once those initial adjustments took
place and transition costs were incurred. ose more sig-
nicant changes would allow individuals with the same
income and similar family characteristics to receive simi-
lar subsidies for health insurance. ey also would reduce
the extent to which subsidies, namely the tax preferences
for employment-based health insurance, increased as
income increased, or eliminate the subsidies altogether.
e approaches that CBO analyzed are as follows:
Approach 1: Partially Subsidized Default Coverage at
Operates in Tandem With Current Sources of Coverage.
is approach would use partially subsidized default cov-
erage to cover all people in a dened population who did

4 Policies to Achieve NeAr-UNiversAl heAlth iNsUrANce coverAge october 2020
Table 1 .
Summary of Approaches to Achieve Near-Universal Health Insurance Coverage Through a Default Plan
Approach Summary Variants Examples
Approach 1:
Partially Subsidized
Default Coverage That
Operates in Tandem
With Current Sources of
Coverage
This approach would provide partially subsidized default coverage through a
private or public plan to cover people who did not actively enroll in an alterna-
tive source of coverage and were not eligible for Medicaid or CHIP. Most key
features of the ACA would remain in place, but premium subsidies would be
extended to those whose income was less than 100 percent of the FPL and
potentially made more generous for middle- and higher-income households.
In addition, the employer firewall would be removed.
a
Private default
plan
Fiedler and others
(2019)
b
Public option
as default plan
Blumberg and others
(2019a)
c
Approach 2:
Partially Subsidized
Default Coverage Through
a Large Public Program
That Replaces Medicaid,
CHIP, and the Nongroup
Market and Retains
Employment-based
Coverage
A new public program consisting of a publicly administered plan and several
private-plan options would replace the existing nongroup market and Medicaid
and CHIP acute care coverage.
d
Large employers would be required to oer
coverage or make mandatory contributions to the public program, and em-
ployees could choose to receive coverage either through their employer or
through the public program. Premium and cost-sharing reductions would remain
income-based and would become more generous. The public plan would provide
partially subsidized default coverage for those without an alternative source of
coverage.
n.a. Medicare for
America Act of 2019
(H.R. 2452); Center
for American Progress
(2019)
e
Blumberg and others
(2019b)
f
Approach 3:
Premium Subsidies for
All People and Default
Coverage Through a Fully
Subsidized Plan
All households would receive a subsidy generous enough to cover the entire
cost of a specified benchmark plan in a marketplace of private plans, potentially
including a public option. Low- and middle-income households would receive
cost-sharing reductions, and supplemental coverage that reduced cost sharing
or provided additional benefits could be obtained through employers. A bench-
mark zero-premium plan would provide fully subsidized default coverage for
those without an alternative source of coverage.
Subsidy covers
catastrophic
plan
Dolan (2019); Gold-
man and Hagopian
(2012)
g
Subsidy covers
generous plan
Halvorson and Oz
(2020); Joyce (2019);
Janda and Ho (2019);
Wynne (2017)
h
Approach 4:
A Single-Payer System
All eligible individuals would be enrolled in a single public plan, typically with
no role for private coverage, and no premiums would be collected. Cost sharing
could be income-based or, as in existing legislative proposals, zero for all
individuals.
n.a. Medicare for All Act
of 2019 (H.R. 1384);
Medicare for All Act
of 2019 (S. 1129)
Source: Congressional Budget Oce.
ACA = Aordable Care Act; CHIP = Children’s Health Insurance Program; FPL = federal poverty level; H.R. = House of Representatives; S. = Senate; n.a. = not applicable.
a. Under current law, people with an aordable oer of employment-based coverage are ineligible for premium subsidies in the health insurance
marketplaces because of a provision of the Aordable Care Act known as the employer firewall. In 2020, an oer of aordable employment-based
coverage is defined by the Internal Revenue Service as one in which an employee’s out-of-pocket premium is less than 9.78 percent of household
income for a single plan. For more details about the employer firewall, see Box 1 on page 22.
b. Rather than extending eligibility for marketplace subsidies to those whose income is below 100 percent of the FPL, the proposal includes features
that would provide incentives for states that have not expanded Medicaid under the terms of the ACA to do so. See Matthew Fiedler and others,
“Building on the ACA to Achieve Universal Coverage,” New England Journal of Medicine, vol. 380, no. 18 (May 2019), pp. 1685–1688, http://doi.
org/10.1056/NEJMp1901532.
c. The proposal also would increase the generosity of marketplace subsidies and establish a federal reinsurance program for the nongroup market.
See “Simulated Reform Packages: Reform 5,” in Linda J. Blumberg and others, From Incremental to Comprehensive Health Insurance Reform: How
Various Reform Options Compare on Coverage and Costs (Urban Institute, October 2019a), p. 6, https://tinyurl.com/yy9atuf7 (PDF, 1.05 MB).
d. The nongroup market is a private health insurance market that enables individuals and families who are not eligible for coverage through public
programs or who do not have employment-based insurance to purchase a private health insurance plan.
e. See Medicare for America Act of 2019, H.R. 2452, 116th Cong. For related information, see Center for American Progress Health Policy Team, Medicare
Extra: Universal Coverage for Less Than $3 Trillion and Lower Health Care Costs for All (July 2019), https://tinyurl.com/yyx9f55d (PDF, 1.18 MB).
f. The proposal does not require large employers to oer coverage or make mandatory contributions. See “Description of Policy Options: The Building
Blocks of Healthy America,” Variant 3: “HA With CARE,” in Linda J. Blumberg and others, The Healthy America Program, An Update and Additional
Options (Urban Institute, September 2019b), p. 3, https://tinyurl.com/y3x3zyrs (PDF, 533 KB).
g. See Ed Dolan, Universal Catastrophic Coverage: Principles for Bipartisan Health Care Reform (Niskanen Center, June 2019), https://tinyurl.com/y4jkfzco
(PDF, 969 KB). See also Dana Goldman and Kip Hagopian, “The Health-Insurance Solution,” National Aairs (Fall 2012), https://tinyurl.com/y3es67tp.
h. See George Halvorson and Mehmet Oz, “Medicare Advantage for All Can Save Our Health-Care System,” Forbes (June 11, 2020), https://tinyurl.
com/yyjvw8j2; Georey Joyce, “Opinion: The Success of Medicare Advantage Makes It a Better Policy Choice Than ‘Medicare for All,’” MarketWatch
(November 21, 2019), https://tinyurl.com/y42cj4zl; Ken Janda and Vivian Ho, “Medicare Advantage for All,” The Hill (August 27, 2019), https://
tinyurl.com/y6avusv8; and Billy Wynne, “The Bipartisan ‘Single Payer’ Solution: Medicare Advantage Premium Support for All,” Health Aairs Blog
(May 11, 2017), https://tinyurl.com/y6xba4hx.

5october 2020 Policies to Achieve NeAr-UNiversAl heAlth iNsUrANce coverAge
Table 2 .
Key Features of Approaches to Achieve Near-Universal Health Insurance Coverage Through a Default Plan
Compared With the System in Eect Under Current Law
Key Feature Current Law
Approach 1:
Establishes
Partially
Subsidized
Default Coverage
a
Approach 2:
Establishes a
Large Public
Program
b
Approach3:
Provides Premium
Subsidies for
All People
c
Approach 4:
Establishes a
Single-Payer
System
Premiums
All eligible individuals have the option of zero-premium
primary coverage
No No No Yes Yes
Premium subsidies are more generous for lower-income
people than for higher-income people
Yes Yes Yes n.a. n.a.
All eligible individuals with income below the federal
poverty level have subsidized coverage
No Yes Yes Yes Yes
Cost Sharing
Cost-sharing reductions are more generous for lower-
income people than for higher-income people
Yes Yes Yes Yes Maybe
Role of Private Plans
All eligible individuals have the option of a private plan Yes Yes Yes Yes No
Role of Employment-Based Coverage
Individuals with an oer of aordable employment-based
coverage are eligible for premium subsidies and cost-
sharing reductions (the “employer firewall” is eliminated)
d
No Yes Yes Yes n.a.
Employers are a large source of primary coverage Yes Yes Maybe No No
Employment-based coverage is eliminated No No No No
e
Yes
Role of Public Coverage
Medicare is preserved for people over the age of 65 Yes Yes Yes Yes No
Medicaid and CHIP are preserved for acute care Yes Yes No No No
All eligible individuals have the option of enrolling in a
public plan
No Maybe Yes Maybe Yes
All eligible individuals are required to enroll in a public plan No No No No Yes
Source: Congressional Budget Oce.
CHIP = Children’s Health Insurance Program; n.a. = not applicable.
a. Approach 1 could be implemented through a variant that introduced a new public option as a source of coverage that also would provide default
coverage for otherwise uninsured people who did not actively enroll in another source of coverage. The new public option could be in the form of a
public plan oered through existing health insurance marketplaces established by the Aordable Care Act.
b. The new public program would allow people to choose between a publicly administered plan and multiple private plans meeting the same minimum
requirements for cost sharing and covered benefits in a health insurance marketplace. Under some existing proposals, the new program also would
replace the current Medicare program.
c. The new system would allow people to use a premium subsidy to choose among multiple private plans in a marketplace. Variations of this approach
also could include a publicly administered plan option alongside the private plans. The new premium support system could exist alongside the
current Medicare program, or it could be combined with the current Medicare program.
d. Under current law, people with an aordable oer of employment-based coverage are ineligible for premium subsidies in the health insurance
marketplaces because of a provision of the Aordable Care Act known as the employer firewall. In 2020, an oer of aordable employment-based
coverage is defined by the Internal Revenue Service as one in which an employee’s out-of-pocket premium is less than 9.78 percent of household
income for a single plan. For more details about the employer firewall, see Box 1 on page 22.
e. The only type of employment-based coverage that would remain under this approach would be for supplemental coverage that could be used
to reduce cost-sharing amounts, or it could be used to oer benefits that are not available through marketplace plans, such as dental and vision
services.

6 Policies to Achieve NeAr-UNiversAl heAlth iNsUrANce coverAge october 2020
not otherwise enroll in a health insurance plan. Default
coverage would be provided by a private or public plan
for people who are ineligible for Medicaid and CHIP;
it would be provided by Medicaid and CHIP to indi-
viduals who are currently eligible for but not enrolled in
those programs. Existing sources of coverage—including
Medicaid, CHIP, employment-based insurance, and
nongroup insurance—and subsidies to purchase health
insurance would remain in place.
is approach would remove the “employer rewall”
provision of the ACA, thus making people with an oer
of aordable employment-based coverage eligible for pre-
mium subsidies—including partially subsidized default
coverage.
2
Most of the other features of the ACA, such as
income-related premium subsidies and insurance market
regulations, would remain in place. is approach also
would extend full premium subsidies to people whose
income was below 100percent of the federal poverty
guidelines (commonly referred to as the federal poverty
level, or FPL), as well as to people whose income fell
below the tax-ling threshold.
3
is approach also could
increase the generosity of subsidies for other households.
Under variants of this approach, default coverage could
be provided by a private plan or through a new pub-
lic option oered through the marketplaces. If default
coverage was provided through a new public option,
that public plan also would be available to all people
who chose to actively enroll during an open-enrollment
period. People who were otherwise uninsured and not
eligible for full subsidies would be assessed a premi-
um-equivalent tax to nance their default coverage. e
amount of that tax would be the same as the premium
2. Under current law, people with an aordable oer of
employment-based coverage are ineligible for premium subsidies
in the health insurance marketplaces because of a provision of
the ACA known as the employer rewall. In 2020, an oer of
aordable employment-based health insurance is dened by the
Internal Revenue Service as one in which an employee’s out-of-
pocket premium is less than 9.78percent of household income
for a single plan.
3. Eligibility for premium tax credits in coverage year 2019 was
based on poverty guidelines for 2018. In 2018, the FPL was
$12,140 for a single person, and that amount increased by
$4,320 for each additional person in a household. People with
income below a certain level, known as the tax-ling threshold,
are not required to le federal income tax returns. In 2019,
the tax-ling threshold for single adults under the age of 65
was $12,200, which was just over the eligibility threshold for
premium tax credits.
the uninsured person would pay to enroll in a bench-
mark plan in the nongroup market that provided equiv-
alent benets, after applying any premium tax credits for
which he or she was eligible. at would preserve incen-
tives for people to actively enroll in other plans, such as
subsidized nongroup plans and employment-based plans
that they might prefer because of those plans’ more gen-
erous benets or broader providernetworks.
Compared with the other approaches CBO analyzed,
this approach would represent the most incremental
change because most features of the current system, other
than the employer rewall, would remain in place. e
transition to the system outlined in this approach would
lead to some changes in sources of coverage. Removing
the employer rewall without imposing additional
penalties or requirements on employers to oer generous
coverage probably would lead some low-income people
who currently receive employment-based coverage to
switch to subsidized coverage through the nongroup
market if they had the option of paying a lower pre-
mium. In addition, some employers might discontinue
oering coverage, leaving their employees to enroll in
the nongroup market. People who are uninsured under
current law would gain coverage, primarily through the
partially subsidized nongroup market or the default plan.
Although this approach demonstrates that attaining
near-universal coverage while retaining existing sources
of coverage is possible, providing default coverage would
be signicantly more challenging to implement than
under other approaches that simplied coverage options
and subsidized premiums to a greater degree. Identifying
the people who were covered by the new default plan
would be particularly complex under this approach
because the government would need to verify the cover-
age status of all eligible people and determine whether
they were eligible for Medicaid or CHIP, which would be
administratively complex.
Approach 2: Partially Subsidized Default Coverage
rough a Large Public Program at Replaces
Medicaid, CHIP, and the Nongroup Market and Retains
Employment-Based Coverage. is approach would
establish a new public program consisting of a publicly
administered plan and several privately administered
plan options to replace the current nongroup market and
the portions of Medicaid and CHIP that cover medical
services and prescription drugs. However, many people
would continue to enroll in employment-based insurance

7october 2020 Policies to Achieve NeAr-UNiversAl heAlth iNsUrANce coverAge
if those plans had lower out-of-pocket premiums,
more-generous benets, or broader provider networks
than the plans oered through the public program.
All low-income people would be eligible for full pre-
mium subsidies to enroll in a public or private plan
through the large public program, and middle-income
people would be eligible for partial premium subsidies
that were more generous than the subsidies available
through the marketplaces under current law. Large
employers would be required to oer private plans or
oer coverage through the public program by making
mandatory contributions on behalf of their employees.
Employees could choose to receive coverage through
the public program (in which case, they could choose
between the private and public plan options oered
through the public program) or through their employer
if the employer continued to oer private coverage.
e public program also would include income-related
cost-sharing reductions for low-income people.
e new public program also would provide partially
subsidized default coverage for all people who did not
otherwise enroll in health insurance coverage. As with
the rst approach, a premium-equivalent tax would
be imposed on middle- and higher-income uninsured
people to nance their default coverage. at tax would
equal the premium people would have paid to enroll in
the public plan, so that low-income people who were eli-
gible for full premium subsidies (including people whose
income is too low to le income tax returns) would not
pay such a tax.
e transition to a system following this approach
would involve more signicant changes than the rst
approach because all people obtaining coverage in the
current nongroup market or through Medicaid or
CHIP would transition to a plan oered through the
new public program. Some people currently enrolled in
employment-based coverage also would transition to the
new public program if they opted for coverage through
the new program rather than through their employer’s
plan, if their employer opted to oer coverage through
the new program, or if their employer stopped oering
coverage altogether. People who were uninsured under
current law would gain coverage, primarily through the
publicprogram.
Approach 3: Premium Subsidies for All People and
Default Coverage rough a Fully Subsidized Plan.
Under this approach, all eligible people under age 65
would receive a premium subsidy that would fully cover
the cost of a benchmark plan (a plan used to determine
subsidies) in a marketplace of private plans. at subsidy
could be provided as a refundable tax credit, which would
reduce revenues and increase outlays, or through direct
payments, which would only increase outlays. Under
some variants of this approach, the subsidy could be less
generous and cover the cost of a catastrophic plan. (Such
health insurance plans, with low premiums and high
deductibles, have an actuarial value of less than 60per-
cent, which means that enrollees are required to pay
for more than 40percent of their health care costs out
of pocket, on average.) Alternatively, the subsidy could
cover the full cost of a benchmark plan that was relatively
generous, similar to a gold plan or the current Medicare
program. (A gold plan is a health insurance plan in the
marketplaces with an actuarial value of about 80percent,
which means that enrollees are required to pay for 20per-
cent of their health care costs out of pocket, on average.)
Another variation of this approach could include a public
plan as an option alongside the private plans.
ere would be no requirements for employers to oer
coverage. Employers would no longer provide primary
health insurance coverage because of the subsidized
private coverage available to their employees, but they
could oer supplemental coverage to reduce cost sharing
or provide additional benets not covered by the plans
their employees chose in the private market. Tax pref-
erences for such supplemental coverage, like those for
employment-based insurance under current law, would
be eliminated. Low- and middle-income households
would receive cost-sharing reductions under all variants
of this approach. All people who did not otherwise enroll
in a plan would receive fully subsidized default coverage
through a benchmark zero-premium plan. e bench-
mark zero-premium plan could have a narrow network
or high cost sharing that would lead some people to
choose to pay more to enroll in a plan with a broader
network or lower cost sharing. Under this approach, peo-
ple’s choice of health insurance plans would be preserved.
e transition to a system that provided full premium
subsidies for all people would involve many more
changes to the current system than the approaches
discussed above because many people would transition
away from employment-based coverage as their primary
source of coverage, and private plans would have to
adapt to a new market. To achieve decit neutrality, large
new sources of tax revenues would be required to nance
universal premium subsidies, in addition to the revenues

8 Policies to Achieve NeAr-UNiversAl heAlth iNsUrANce coverAge october 2020
raised because tax preferences for employment-based
coverage would be eliminated and a greater share of
employees’ compensation would be taxed.
Once the new system was established, implementation
of default coverage generally would be simpler than with
the approaches already discussed because there would
be no need to collect premium-equivalent tax payments
from people who would be covered automatically by
a zero-premium default plan. Also, people would not
need to change their coverage when they changed jobs or
experienced a change in income.
Approach 4: A Single-Payer System. Under this
approach, the government would enroll all eligible peo-
ple in a single-payer system, and in all existing proposals
using this approach, there generally would be no role, or
there would be a very limited role, for private insurance.
If private insurance was allowed, it most likely would
be limited to services not covered by the public plan.
Private insurance also could be oered as an alternative
source of coverage if some enrollees and providers were
allowed to opt out of the single-payer system. Cost shar-
ing under this approach typically would be lower than
under current law. ere would be no premiums, and to
achieve decit neutrality, such a system would need to be
nanced with broad-based tax revenues.
e transition to a single-payer system would involve
greater changes for individuals, insurers, and health care
providers than the other approaches, and it would be
an enormously complex undertaking. To achieve decit
neutrality, large new sources of tax revenues would be
required to nance the single-payer system, and new
nancing mechanisms would need to be established.
However, once it was established and people obtained
proof of enrollment, they would be covered under the
same system for the rest of their lives.
Background and Scope of the Report
Under the current multipayer health care system, people
under the age of 65receive health insurance from a
variety of public and private sources, most of which are
partially subsidized by the federal government. at sys-
tem has not resulted in near-universal health insurance
coverage because not everyone is eligible for subsidized
coverage—even people with very low income—and not
everyone who is eligible for subsidized coverage chooses
to purchase it. Lawmakers have considered a variety of
proposals to decrease health insurance premiums and
increase the number of people with coverage. However,
many of those proposals are not comprehensive enough
to achieve near-universal coverage.
ree broad strategies for establishing a health insurance
system would achieve near-universal coverage: enacting
and enforcing a large individual mandate penalty, insti-
tuting automatic coverage through a default plan, or cre-
ating a single-payer system that would serve as a default
plan for all people. All of those strategies would require
generous subsidies for the low- and moderate-income
people for whom the cost of health insurance would
typically be prohibitive. In this report, CBO does not
describe approaches that would achieve near-universal
coverage by using an individual mandate penalty because
the agency could nd no recent proposals that would
do so and because the Congress recently eliminated the
individual mandate penalty that was established under
the ACA.
Denition of Health Insurance Status and Coverage
CBO considers people who enroll in a private health
insurance plan or a government program that provides
comprehensive major medical coverage to be insured.
Such coverage protects people against high-cost medical
events, but it still could result in hundreds or thou-
sands of dollars in out-of-pocket costs if it required
signicant cost sharing, such as a high deductible (an
amount a patient is required to pay before a plan begins
covering any costs) or large copayments (xed dollar
amounts that a patient is required to pay when using
particularservices).
CBO considers people who are not enrolled in such a
plan or program to be uninsured—even if they are eligible
to immediately enroll in a plan or government program
that would pay for any previously incurred health care
expenses retroactively upon enrollment. For example, peo-
ple who are eligible for but not enrolled in Medicaid have
an implicit protection against high-cost medical events
because they can enroll in that program at any time, and
they may have retroactive coverage for expenses incurred
before enrollment. However, CBO still classies those
people as uninsured. In CBO’s view, that denition of
uninsured aligns with the concept underlying data from
the National Center for Health Statistics, which relies on
individuals to report their insurance status in surveys.
4
4. For previous discussion of related issues, see Congressional
Budget Oce, Health Insurance Coverage for People Under Age
65: Denitions and Estimates for 2015 to 2018 (April 2019),
www.cbo.gov/publication/55094.

9october 2020 Policies to Achieve NeAr-UNiversAl heAlth iNsUrANce coverAge
Although this report refers to all people who are not
enrolled in a comprehensive major medical insurance
plan or a government program as uninsured—to be
consistent with typical denitions—it recognizes that
those otherwise uninsured people would have some
nancial protection against high-cost medical events
if they had automatic coverage through a default plan.
Consequently, in this report, CBO refers to people who
are not enrolled in a plan but have automatic coverage
through a default plan as having coverage and counts
them when assessing the universality of coverage. e
tension of describing a group of people as uninsured yet
having coverage reects the complexity that arises when
people receive nancial protection against high-cost
medical events without enrolling in an insurance plan.
Such people also could have diculty accessing care in
the absence of a connection to a health insurance plan
and provider network and might forgo some care, such
as preventive services.
As classied by CBO, a policy would achieve near-uni-
versal coverage if close to 99percent of citizens and
non citizens who are lawfully present in the country were
covered either by enrolling in a comprehensive major
medical plan or by receiving automatic coverage through
a default plan. In addition, a policy could achieve
near-universal coverage of all U.S. residents if nonciti-
zens who are not lawfully present also were made eligi-
ble for coverage. Policymakers might allow for limited
exemptions, such as for people with religious or moral
objections.
In CBO’s assessment, no existing proposals would
achieve complete (that is, 100percent) universal cover-
age because they all would require some demonstration
of eligibility (such as meeting criteria related to citizen-
ship or residency) that some eligible people would not
comply with for various reasons. For example, some peo-
ple would not comply because of language and literacy
barriers or fears of providing information to the federal
government. By CBO’s classication, a health care
system would achieve complete universal coverage only if
all people in the country received coverage without any
required demonstrations of eligibility criteria.
Sources of Coverage and Uninsured People
Under Current Law
In the current multipayer system, people obtain health
insurance from a variety of private and public sources.
Most uninsured people have at least one subsidized
option available to them, but others have no subsidized
option and purchasing health insurance can cost a large
share of their income.
Sources of Health Insurance. Under current law, people
under the age of 65receive coverage through three major
sources: employment-based health insurance, public pro-
grams such as Medicaid and CHIP, and nongroup health
insurance for those who do not obtain health insurance
through their employer and do not qualify for public
programs. ose three sources all provide comprehensive
major medical coverage and require no cost sharing for
preventive care services, such as vaccinations. (A small
number of people in the nongroup market are enrolled
in plans that do not provide comprehensive major med-
ical coverage. CBO does not consider those plans to be
insurance.)
However, the amount of cost sharing required for
nonpreventive care and the network of participating
providers vary. Employment-based plans tend to have
greater cost sharing requirements and a broader network
of participating providers than Medicaid. Medicaid
and CHIP require no or very limited cost sharing, but
many providers do not participate in those programs.
Nongroup plans tend to require even higher cost sharing
than employment-based plans, and they can have a more
limited network of participating providers. However,
nongroup plans—including those available both in and
outside of the health insurance marketplaces established
under the ACA—vary considerably in their levels of
costsharing.
Plans in the nongroup market that provide comprehen-
sive major medical coverage are classied according to
their level of cost sharing using “metal tiers,” with more
precious metals (for instance, gold) indicating lower
levels of cost sharing but higher premiums. For example,
a typical silver plan has an actuarial value of 70per-
cent, which means that enrollees are required to pay for
30percent of their health care costs out of pocket, on
average. By contrast, a typical gold plan has an actuar-
ial value of 80percent, which means that enrollees are
required to pay for only 20percent of their health care
costs out of pocket, on average. ose dierences in cost
sharing can be seen by comparing average deductibles. In
2019, an average bronze plan had a deductible of about
$6,300, while an average gold plan had a deductible of
about $1,300.
5
e silver plans with cost-sharing reduc-
5. See Kaiser Family Foundation, “Cost-Sharing for Plans Oered
in the Federal Marketplace, 2014–2020” (December 2019),
https://tinyurl.com/y448slxf.

10 Policies to Achieve NeAr-UNiversAl heAlth iNsUrANce coverAge october 2020
tion (CSR) subsidies require even less cost sharing. ose
subsidies are available through the health insurance mar-
ketplaces to people with income between 100percent
and 250percent of the FPL.
People whose income is between 100percent and
400percent of the FPL and who are not eligible for
public coverage and do not have access to an oer of
aordable employment-based coverage are eligible for
premium subsidies to purchase nongroup plans through
the health insurance marketplaces. People with an aord-
able oer of employment-based coverage are ineligible
for such subsidies because of the employer rewall. (In
2020, an oer of aordable employment-based coverage
is dened by the Internal Revenue Service, or IRS, as
one in which an employee’s out-of-pocket premium is
less than 9.78percent of household income for a single
plan.) e amount of those subsidies is benchmarked to
the cost of the second-lowest-cost silver plan, and it is
based on aordability thresholds that vary by income.
For example, people with the lowest income receive pre-
mium subsidies that allow them to purchase that bench-
mark plan for 2.06percent of their income. People with
higher income receive smaller subsidies that require them
to pay 9.78percent of their income for the same plan.
Options Currently Available to Uninsured People. In
2019, an estimated 30million people under the age of
65, or 12percent of that population, were uninsured.
One reason for the lack of insurance coverage was a lack
of subsidized options. About one-third of uninsured peo-
ple under the age of 65did not have access to coverage
that was subsidized by the government or an employer:
13percent were noncitizens who were not lawfully
present in this country; 11percent had income that was
less than 100percent of the FPL and lived in a state that
did not expand Medicaid; and 9percent had income
that was too high to qualify for marketplace subsidies
(see Figure 1). Many of those people, including nearly
all of the people in the rst two groups, would have to
pay large premiums relative to their income to enroll in a
health insurance plan.
6
Another reason for the lack of health insurance cover-
age is that not all people who are eligible for subsidized
coverage choose to purchase it. About two-thirds of the
30million uninsured people under the age of 65 had
access to some form of subsidized coverage but were
not enrolled, although those options were subsidized to
6. See Congressional Budget Oce, Who Went Without Health
Insurance in 2019, and Why? (September 2020), www.cbo.gov/
publication/56504.
Figure 1 .
Eligibility for Subsidized Coverage Among Uninsured People in 2019
Made
Eligible for
Medicaid
by the ACA
Otherwise
Eligible for
Medicaid
or CHIP
Eligible for
Marketplace
Subsidies
a
Eligible for Subsidized
Employment-Based
Coverage
b
Not
Lawfully
Present
Income Below
FPL in a State
That Did Not
Expand
Medicaid
Income
Too High for
Marketplace
Subsidies
Eligible for Subsidized Coverage
20.0 Million, 67 Percent
Not Eligible for Subsidized Coverage
9.8 Million, 33 Percent
2.2
Million,
7%
2.9
Million,
10%
5.5
Million,
19%
9.4
Million,
31%
4.0
Million,
13%
2.6
Million,
9%
3.2
Million,
11%
Source: Congressional Budget Oce.
Some people may be eligible for multiple sources of coverage. CBO classified uninsured people into mutually exclusive groups on the basis of the most
heavily subsidized option available to them or the primary reason they were ineligible for subsidized coverage.
CBO’s estimates of the number of uninsured people and their options for coverage were drawn from its health insurance simulation model, HISIM2, and
may dier from other sources. For more details about those estimates, see Congressional Budget Oce, Who Went Without Health Insurance in 2019,
and Why? (September 2020), www.cbo.gov/publication/56504.
ACA = Aordable Care Act; CHIP = Children’s Health Insurance Program; FPL = federal poverty level.
a. A small number of people in this group would technically be eligible for subsidies, but those subsidies would equal zero dollars.
b. A small number of people in this group were self-employed and could receive a subsidy by deducting their premiums from their income when
calculating their federal income taxes.

11october 2020 Policies to Achieve NeAr-UNiversAl heAlth iNsUrANce coverAge
dierent degrees: 17percent were eligible for Medicaid
or CHIP; 19percent were eligible for subsidized cov-
erage through the marketplaces established under the
ACA; and 31percent had access to coverage through an
employer. Most of those people could have purchased
health insurance that cost less than 10percent of their
income, but fewer people had an option that cost less
than 5percent of their income. ose people lacked
health insurance coverage because they did not consider
it to be worth the cost or because of the complexities of
the enrollment process, among other reasons.
Legislative Proposals to Incrementally Expand Access
to Coverage and Reduce Out-of-Pocket Premiums
Lawmakers have introduced legislative proposals that
would reform health insurance in various ways. Such
proposals generally include provisions that would incre-
mentally expand access to coverage by providing people
additional plan options, increasing subsidies, or reducing
out-of-pocket premiums in other ways. For example,
some legislative proposals have been introduced in the
current Congress that would expand subsidies to dif-
ferent income groups, introduce a public option in the
health insurance marketplaces, or allow people to buy
in to public programs.
7
Although legislation that would
reduce out-of-pocket premiums would result in expanded
access to partially subsidized coverage and encourage
more people to enroll in a plan, it would not by itself
achieve near-universal coverage because some people
would choose not to purchase health insurance. ose
people would not otherwise have nancial protection
against high-cost medical events.
Expansion of Subsidies. Some legislative proposals, such
as H.R. 1425, the Patient Protection and Aordable
Care Enhancement Act, would reduce out-of-pocket
premiums by expanding the subsidies available under
current law to people whose income is above 400per-
cent of the FPL and encourage more people to enroll in
a plan. at bill also would make the premium subsi-
dies under current law more generous by reducing the
amount of income that people must contribute toward
their premiums. In addition, the proposal would elim-
inate the provision of the ACA that prevents low- or
moderate -income people from receiving subsidies if a
7. For a comparison of some proposals, see Kaiser Family
Foundation, “Compare Medicare-for-All and Public Plan
Proposals” (May 15, 2019), www.k.org/interactive/
compare-medicare-for-all-public-plan-proposals.
worker has an oer of aordable employment-based
coverage for a singleplan.
Public Option. Under legislative proposals that
would establish a public option—such as S. 3, the
Keeping Health Insurance Aordable Act of 2019, and
H.R. 2085, the CHOICE Act—a new public plan
would be oered in the health insurance marketplaces
alongside private plans, and providers’ payment rates
would be set by the government. Some other proposals
also would oer a public option in the individual and
small-group markets outside of the marketplaces. Such
proposals aim to reduce premiums and provide people
with additional plan options.
Medicare Buy-In. Under legislative proposals that
would establish a Medicare buy-in—such as S. 470,
the Medicare at 50Act, and H.R. 1346, the Medicare
Buy-In and Health Care Stabilization Act of 2019—
certain older adults under the age of 65who are not cur-
rently eligible for Medicare would be allowed to purchase
coverage through that program. ose proposals also
would allow marketplace subsidies to be used toward the
purchase of that coverage for people who were eligible
for subsidies, and they would provide some people with
additional plan options that had lower premiums than
current nongroup options.
Medicaid Buy-In. Under legislative proposals that
would establish a Medicaid buy-in, such as S.489 and
H.R. 1277, the State Public OptionAct, people at all
income levels would be allowed to purchase coverage
through participating state Medicaid programs. Such pro-
posals would not require states to adopt that program—
similar to states’ voluntary participation in the Medicaid
program more broadly. Under this approach, a Medicaid
buy-in program would be oered in the health insurance
marketplace alongside private plans, and marketplace
subsidies could be used toward the purchase of a Medicaid
buy-in for people who were eligible for subsidies. Such
proposals would provide some people with additional plan
options that would have lower premiums than current
nongroup options.
Strategies to Achieve Near-Universal Coverage
Under all three strategies—a large and enforced indi-
vidual mandate penalty, automatic coverage through
a default plan, and a single-payer system—gener-
ous subsidies would be required to assist low- and

12 Policies to Achieve NeAr-UNiversAl heAlth iNsUrANce coverAge october 2020
moderate income people for whom the cost of health
insurance would typically be prohibitive, and a manda-
tory component would be necessary to ensure that peo-
ple did not forgo coverage. In contrast with current law,
people would not be able to remain uninsured during
periods in which they did not anticipate using health
care services and enroll in a health plan only after they
anticipated or experienced a high-cost medical event.
Large and Enforced Individual Mandate Penalty. One
way to provide coverage to nearly all people under a mul-
tipayer system would be to combine generous premium
subsidies with a requirement that everyone purchase
health insurance. To be eective, that requirement would
have to be strongly enforced, and people who did not
comply would incur large nancial penalties. Such a
strategy is used by several European countries, including
Germany and the Netherlands, that have near-universal
coverage through highly regulated multipayer systems.
e ACA combined an individual mandate with an
increase in subsidized coverage options. However, the
ACA did not result in near-universal coverage because
the nancial penalties for the individual mandate were
modest and only partially enforced and because some
low-income people, particularly low-income adults
below the FPL in states that did not expand Medicaid,
were not made eligible for the new subsidized coverage
options. (For example, the ACA prohibited the use of
liens or levies by the IRS to collect the nancial penalties
for not complying with the individual mandate, and
people could not be prosecuted for failing to pay the
penalty. However, the IRS could oset the nancial pen-
alty with any tax refund owed to a person.)
8
In addition,
the Congress later eliminated the nancial penalty for
not complying with the individual mandate in Public
Law115-97, referred to here as the 2017tax act.
Automatic Coverage rough a Default Plan. In the
absence of a large and strongly enforced individual
mandate penalty to induce people to purchase coverage,
another strategy to achieve near-universal coverage would
be to combine premium subsidies with a mechanism that
automatically provided coverage through a default plan.
One strategy used by several countries with near-uni-
versal coverage is a single-payer system that serves as a
8. See Internal Revenue Service, Questions and Answers on the
Individual Shared Responsibility Provision (June2020), https://
go.usa.gov/xGbSD.
default plan. A single-payer system is an extreme example
of a default plan because people would not have a choice
of a health insurance plan and everyone who was eligible
would be enrolled in the same public plan. Automatic
coverage through a default plan also could be used in a
multipayer system that fully subsidized the cost of health
insurance premiums while still allowing people to choose
from among multiple privateplans.
Such a default coverage mechanism also could be used
to achieve near-universal coverage under a multipayer
system that did not fully subsidize the cost of health
insurance for all people, as is the case in Switzerland.
However, the system would become signicantly more
complex for the government to administer because it
would need a way to identify and collect payments
from people who chose not to enroll in a plan and were
not eligible for full subsidies.
9
ose people would be
required to make a payment if they did not enroll in any
source of coverage, as would be the case under a system
that used an individual mandate penalty. However,
they would receive health insurance coverage through a
default plan for any period in which they did not have
another source of coverage—which is dierent from
what would occur under a system that used an individ-
ual mandate penalty (in which a person is liable for a
tax payment but not covered by insurance). Using the
default plan, otherwise uninsured people could receive
covered health care services at any time, without waiting
for an open enrollment period.
Single-Payer System. A third strategy to achieve
near-universal coverage would entail establishing a
single-payer system. As discussed above, a single-payer
system could serve as a default plan and all people who
demonstrated eligibility would enroll in that program
and receive care that was covered by the single-payer
system. A single-payer system is included here as a
separate strategy because, unlike a default plan under a
multipayer system, the government would operate the
single-payer system, and it would determine payment
rates for health care providers. Premiums would be fully
subsidized through broad-based tax revenues. Such a
9. See Ewout van Ginneken and omas Rice, “Enforcing
Enrollment in Health Insurance Exchanges: Evidence From the
Netherlands, Switzerland, and Germany,” Medical Care Research
and Review (April 2015), vol. 72 no. 4, pp. 496–509, https://
doi.org/10.1177/1077558715579867.

13october 2020 Policies to Achieve NeAr-UNiversAl heAlth iNsUrANce coverAge
strategy is used by several countries, including Canada,
Denmark, and the United Kingdom.
10
Scope of the Report
is report discusses the primary features of four general
approaches that could achieve near-universal coverage
using a combination of premium subsidies and automatic
coverage through a default plan, including a single-payer
system. e role of default coverage would vary across
each of the four approaches, but in all cases, a default
plan would provide coverage to people during periods
in which they did not have another source of coverage,
whether or not they used any health care services during
the year. CBO focused on approaches that would achieve
near-universal coverage by using the strategy of automatic
coverage through a default plan, rather than by using
large and strongly enforced individual mandate penal-
ties, because the Congress recently eliminated the ACA’s
individual mandate penalty.
11
CBO is not aware of any
current detailed proposals that would reinstate an indi-
vidual mandate penalty that would be strongly enforced
and large enough to result in near-universal coverage.
Policymakers would need to specify numerous details
in drafting legislation that followed any of those
approaches, and this report does not address every aspect
that would need to be specied. For example, the report
does not discuss the extent to which noncitizens who are
not lawfully present would be eligible for subsidized cov-
erage. is report focuses on how expansions of health
insurance coverage could achieve the goal of near-univer-
sal coverage; a discussion of how the subsidies for those
coverage expansions would be nanced is outside the
scope of the report. e report also does not include esti-
mates of the budgetary eects of any of the approaches
because those eects would vary considerably under
dierent variants of the approaches and would depend
on how numerous other details were specied.
10. For additional discussion of single-payer systems, see
Congressional Budget Oce, Key Design Components and
Considerations for Establishing a Single-Payer System (May 2019),
www.cbo.gov/publication/55150; and Chris Pope, Medicare for
All? Lessons From Abroad for Comprehensive Health-Care Reform
(Manhattan Institute, November 2019), https://tinyurl.com/
tqq9d52.
11. For CBO’s analysis of the eect of the ACA’s individual mandate
penalty, see Congressional Budget Oce, Repealing the Individual
Health Insurance Mandate: An Updated Estimate (November
2017), www.cbo.gov/publication/53300.
Automatic Coverage Through a Default Plan
for People Without an Alternative Source of
Health Insurance: Design Considerations
and Challenges
All four approaches discussed in this report would make
use of a default plan to achieve near-universal coverage.
e role of the default plan would vary on the basis of
the design and other features of the policy approach.
e dening feature of each type of default coverage is
that everyone without an alternative source of insurance
could receive covered care—including comprehensive
major medical services and prescription drugs—at any
time, without waiting for an open-enrollment period.
Some features of the default coverage would depend on
the answers to the following questions: Would default
coverage be partially subsidized and require mandatory
contributions from uninsured people who are eligible for
such coverage, or would it be fully subsidized through
broad-based tax revenues? How heavily subsidized would
the default coverage be if it was only partially subsidized?
And, would default coverage be provided through a
private or public plan?
Implementing default coverage would present particu-
lar challenges if it was partially subsidized. Additional
challenges would arise if the default plan was included in
a risk-adjustment system that shared the cost of insuring
a group of enrollees with other plans that were available
for active enrollment. ere also would be challenges
associated with informing people about their eligibility
for default coverage and the benets associated with that
coverage, particularly the default plan’s provider network.
Enrollment in a Default Plan and Use of
Health Care Under That Plan
e default plan would provide coverage to everyone
during periods in which they did not have an alternative
source of insurance, whether or not they used any health
care services or actively initiated coverage during the
year. e key feature of default coverage is that eligi-
ble people could enroll in the default plan and receive
covered health care services at any time, without waiting
for an open-enrollment period. To use the default plan to
receive covered health care services, people could enroll
in the plan in one of three ways:
•
Point-of-Service Enrollment. Certain health care
providers would be authorized to enroll their
patients at the point of service, which means that

14 Policies to Achieve NeAr-UNiversAl heAlth iNsUrANce coverAge october 2020
an uninsured person seeking care through those
providers would receive health care covered by the
default plan without any prior active enrollment. e
providers that facilitated such enrollment would be
similar to the providers—for instance, most hospitals
and certain other safety-net providers such as
community health centers—that currently assist with
the enrollment of uninsured patients in Medicaid
and CHIP (when they are eligible). For example, a
person who sought care in a hospital emergency room
or medical clinic would be signed up for coverage by
the provider at that time. e provider would bill the
default plan for payment, minus any required patient
cost sharing, for any patient who did not provide
proof of enrollment in another source of health
insurance. Other providers that agreed to participate
in the default plan would accept payment from the
default plan, but they would rst require patients to
enroll in and provide proof of default coverage before
seeking care.
•
Self-Enrollment. Individuals could actively enroll at
any time in a default plan through an online portal
or an alternative process. Under such a process, they
would receive proof of coverage and information on
the benet package, provider network, and other
features of the default plan. at would allow the
person to make an appointment with any health care
provider in the default plan’s network and to present
proof of enrollment as a source of payment at any
participating provider.
•
Automatic Enrollment. Some people could be enrolled
automatically in the default plan and then informed
of their enrollment. Automatic enrollment would
be more feasible for people who were eligible for full
premium subsidies if the government had sucient
information about their income eligibility and
coverage status.
Default Coverage Under Medicaid and CHIP. Medicaid
and CHIP provide default coverage under current law
for some low-income adults and children, with no
waiting period to enroll in those programs. For Medicaid
and some CHIP programs, certain providers are autho-
rized to enroll people who appear to be eligible for those
programs on a presumptive basis at the point of ser-
vice using a simplied income screen. For example, an
uninsured person who visits an emergency room today
can be enrolled in Medicaid by the hospital on the basis
of a simplied income screen, if he or she appears to be
eligible. In many states, people who enroll in Medicaid
also can receive retroactive coverage for up to three
months before their application date for any medical
expenses incurred during that period. at retroactive
coverage removes the nancial liability from individu-
als for the three-month period and allows providers to
receive payment for services that are rendered before
those individuals can submit a complete application.
However, many people may not be aware that they are eli-
gible for Medicaid or CHIP, or that the presumptive and
retroactive eligibility policies exist. As a result, those peo-
ple may be less likely to seek health care than people who
are enrolled and know they have coverage. If a default
plan was available to all otherwise uninsured people, those
people might be more aware of the option of accessing
health care that was paid for by a default plan and more
likely to seek care as a result than uninsured people who
are eligible for Medicaid and CHIP under current law.
Dierences Between Automatic Enrollment in a
Default Plan and Automatic Coverage by at Plan.
Under all four approaches discussed in this report, a
default plan would provide automatic coverage to all eli-
gible but otherwise uninsured people even if they never
enrolled in a plan. Each approach also could make use of
automatic enrollment in other types of health insurance to
minimize the number of eligible people who never enroll
in a plan. Automatic enrollment identies eligible people
and registers them for coverage, typically when no premi-
ums are required. However, many uninsured people are
not eligible for zero-premium options under current law,
and identifying eligible uninsured people to auto-enroll
would be challenging. Automatic enrollment typically
applies on a prospective basis, meaning that people gain
coverage only after they are identied as uninsured and
their enrollment is processed, which could be many
months after they become uninsured. By contrast, auto-
matic coverage does not require identifying uninsured
people at the moment they become uninsured.
Under automatic enrollment, more people would be
enrolled in coverage than under current law, but eligible
people who could not be automatically enrolled would
not be covered, and people who were automatically
enrolled would generally have coverage only after their
enrollment was processed. In CBO’s assessment, it would
be extremely dicult to identify and automatically enroll
otherwise uninsured people when they owed premiums,
and millions of people would remain uninsured unless
a default plan that provided automatic coverage also

15october 2020 Policies to Achieve NeAr-UNiversAl heAlth iNsUrANce coverAge
was established. Most Medicaid and some CHIP enroll-
ees would have retroactive coverage for any expenses
incurred up to three months before enrollment, but peo-
ple automatically enrolled in marketplace plans would
have no such protections under current law.
Under automatic coverage, all people without other
sources of health insurance would be covered by a default
plan. Expanding the use of automatic enrollment in
public and private coverage would increase the number
of people who were enrolled in a health insurance plan
throughout the year and potentially reduce the number
of remaining uninsured people who would be responsible
for tax payments to nance default coverage. However,
if an automatic coverage mechanism was not in place,
the approach would not reach near-universal cover-
age because some people could not be auto-enrolled.
(Other analysts use dierent terminology to refer to
automatic coverage through a default plan, including
retroactive coverage by a backstop plan and continuous
auto-enrollment with retroactive enforcement.)
Key Design Choices Associated With Default Coverage
Proposals to establish default coverage would require
several key design choices, including the extent to which
coverage would be subsidized and whether it would be
provided by a private or a public plan. Another design
choice would center on the degree of cost sharing that
would be required under the default plan.
Partially or Fully Subsidized Default Coverage? A key
design choice for establishing default coverage would
be how heavily to subsidize the cost of that coverage for
otherwise uninsured people who would be covered by
the default plan. If default coverage was partially sub-
sidized, some people in the eligible population, such as
those with low income, would receive a subsidy to cover
the entire cost of a benchmark plan while other people
in the eligible population, such as middle-income people
and some high-income people, would receive a subsidy
to partially cover the cost of a benchmark plan; other
high-income people would not be eligible to receive any
subsidies. Financing would come, in part, from higher
taxes on those uninsured individuals who were cov-
ered by the default plan and, in part, from broad-based
tax revenues that were not linked to health insurance
coverage. Default coverage would be partially subsidized
under Approaches 1 and 2, both of which would subsi-
dize the entire cost of a benchmark plan for low-income
people, but it would provide only partial subsidies for
middle-income and some higher-income people.
Levying taxes on uninsured people who were covered
by the default plan would be the equivalent of charging
mandatory premiums for that coverage. To maintain
incentives to enroll in other sources of coverage, the
amount of the tax associated with default coverage would
be made equal to the net premium the individual would
pay to actively enroll in a benchmark plan providing
the same benets. However, some people would choose
to continue enrolling in employment-based coverage or
other types of plans if those plans included a broader
network or more generous benets.
Some proposals refer to nancing for a default plan as
retroactive premiums because the funds collected at
the end of the year would serve as payment for default
coverage provided during the previous year. Legislation
specifying such nancing as a tax would increase the
likelihood that those payments would be upheld as
constitutional. Although those people would be required
to make a payment if they did not enroll in any source
of coverage—as was the case with the ACA’s individual
mandate penalty—they also would receive health insur-
ance coverage through a default plan for any period in
which they did not have another source of coverage.
e amount of the premium-equivalent tax could vary
on the basis of income or other criteria. For example,
if partially subsidized default coverage was added to
existing sources of coverage and subsidies, the bench-
mark plan could be a silver plan available through the
health insurance marketplaces. e amount of the
premium-equivalent tax would then be the premium
uninsured people would pay to enroll in that silver plan
after applying any premium tax credits for which they
were eligible.
If default coverage was fully subsidized for all eligi-
ble people, everyone in the eligible population would
receive a subsidy to cover the entire cost of a bench-
mark plan. Such coverage would be implemented under
Approaches 3 and 4. Financing would come entirely
from broad-based tax revenues, and people who did not
enroll in a health insurance plan would not owe addi-
tional taxes.
A Private or Public Default Plan? Proposals would need
to specify whether default coverage would be provided
through a private or a public plan. If a private or public
plan in the marketplace served as a default plan, all plans
in the nongroup market would adjust their premiums
to reect the expected costs of adding enrollees through

16 Policies to Achieve NeAr-UNiversAl heAlth iNsUrANce coverAge october 2020
the default coverage mechanism to the existing risk-
adjustment system. If default coverage was provided by
a private plan, a government agency would receive tax
revenues to nance default coverage and use those reve-
nues to make periodic premium payments to the private
default plan for each person estimated to be covered by
that plan. e legislation might specify the characteristics
of the private plan that would be designated to serve as
the default plan—such as the least expensive silver plan
oered in the health insurance marketplace. A private
default plan also could be identied through a compet-
itive bidding process, with plans submitting premium
bids on the basis of the expected costs of providing
coverage to people who would be enrolled through the
default coverage mechanism.
If the default plan was a public plan, such as a new
public option oered through the marketplaces, the
government would set the premium in one of two ways:
on the basis of the expected costs of providing coverage
to people who would enroll through the marketplaces
and the default coverage mechanism, as well as the costs
of any risk-adjustment payments; or on the basis of
private-market estimates of the cost of insuring a person
of average health status, such as the benchmark premium
of the second-lowest-cost silver plan in the marketplace.
Other plans would adjust their premiums if the public
default plan was part of the same risk-adjustment system.
If default coverage was provided by a private plan, pro-
vider networks and payment rates could be negotiated by
insurers and providers, subject to existing requirements
about network adequacy. If default coverage was pro-
vided by a public plan, administrators could set payment
rates, establish criteria regarding provider participation,
and impose other requirements based on those used by
the Medicare program or develop new approaches.
Under variants of Approaches 1 and 3, the default plan
would be a private plan. Default coverage also could be
provided by a public plan, such as a new public option
under one variant of Approach 1. A public plan also
would serve as the default plan under Approach 2, one
variant of Approach 3, and Approach 4.
Default coverage could vary on the basis of the charac-
teristics of the population. For example, Medicaid and
CHIP could continue to serve as default coverage for
people who were eligible for but not currently enrolled in
those programs, and another private or public plan could
serve as default coverage for other uninsured individuals
who were not eligible for Medicaid or CHIP (as under
Approach 1).
Other Design Choices. Other design choices for default
coverage would include the degree of cost sharing that
individuals would be responsible for when using care
under the default plan. e generosity of the default
plan could aect the size of the premium-equivalent tax
for people whose coverage was not fully subsidized. For
example, if a gold plan was specied as the default plan,
all people who were enrolled in the plan would have lower
cost sharing than if they were enrolled in a catastrophic
plan, but people who were not eligible for subsidies would
owe a larger amount in premium-equivalent taxes.
Key Challenges of Implementing Default Coverage
e key challenges of implementing default coverage are
as follows: how to ensure that the appropriate premium-
equivalent tax payments are collected if default coverage
is partially subsidized; how to determine the appropriate
premium adjustments for plans when the default plan
is part of a risk-adjustment system; and how to inform
people about their eligibility for default coverage and the
default plan’s benets, particularly the provider network.
Implementing default coverage would be less admin-
istratively complex if the requirements for assessing
premium-equivalent taxes to nance default coverage
were straightforward and fewer alternative sources of cov-
erage were available. For example, implementing default
coverage in a single-payer system (as in Approach 4)
would present the fewest challenges relative to other
approaches because coverage would be fully subsidized
through broad-based tax revenues and the government
would not need to verify enrollment in other sources of
coverage. However, a single-payer system would result in
the largest increase in government spending.
Implementing partially subsidized default coverage that
operated in tandem with currently available sources of
coverage (including Medicaid, CHIP, employment-based
insurance, and private nongroup insurance) would
present the most challenges relative to other approaches.
at is because the government would need to verify
enrollment using data from many potential sources of
coverage and collect premium-equivalent tax payments
from people who were not enrolled in those other plans
or programs.
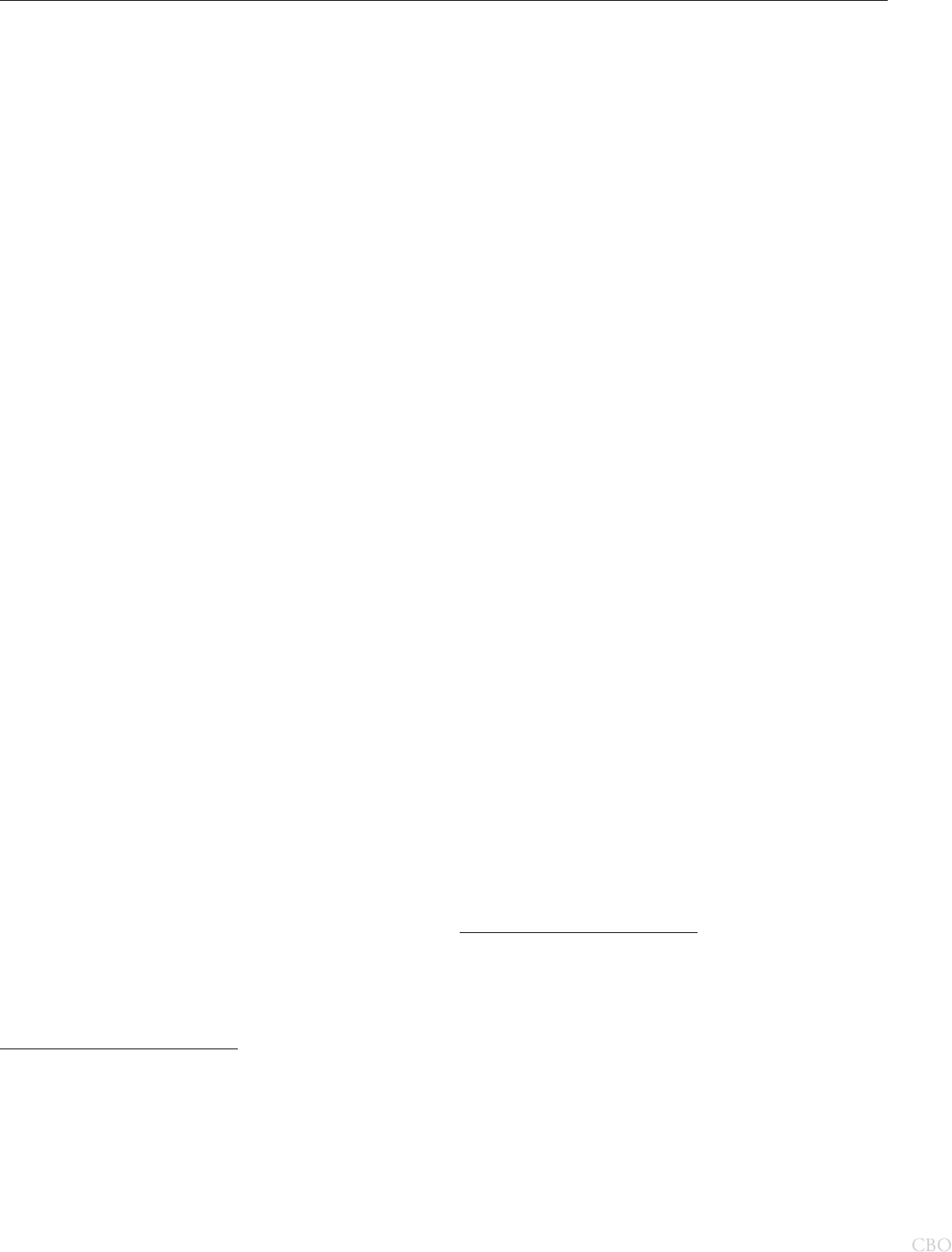
17october 2020 Policies to Achieve NeAr-UNiversAl heAlth iNsUrANce coverAge
Collecting Premium-Equivalent Taxes When Default
Coverage Is Partially Subsidized. Under Approaches 1
and 2, which would provide partially subsidized default
coverage, the government would collect premium-equiv-
alent taxes from people who were covered by the default
plan because they did not have an alternative source of
coverage. Collecting those taxes would be challenging for
several reasons. First, in many cases, it would be dicult
to determine which people did not have an alternative
source of coverage and therefore were responsible for pre-
mium-equivalent taxes. Second, the tax payments would
be large for higher-income people without other sources
of coverage who were eligible for small or no subsidies.
ird, both of the two main options for structuring the
taxes would add additional complexity to the tax system
and would make withholding the appropriate amount
of taxes from workers’ paychecks throughout the year
moredicult.
Identifying People Responsible for Paying Premium-
Equivalent Taxes. Under Approaches 1 and 2, the IRS
would need to identify the coverage status of all income
tax lers and determine their eligibility for premium
subsidies in order to collect premium-equivalent taxes.
When tax returns were led, each person’s insurance
status and eligibility for subsidized coverage would
be assessed for each month of the previous calendar
year.
12
For each month that an individual did not have
an alternative source of coverage, the person would be
considered to have been covered by the default plan and,
depending on that person’s income and eligibility for
premium subsidies, he or she would owe additional tax
payments. If default coverage was partially subsidized,
the premium-equivalent tax would be set equal to the
premium of the default plan minus any premium tax
credits or subsidies for which the person was eligible.
e IRS would determine coverage status on the basis
of self-reported information that would be veried by
matching it to information submitted by third parties
(such as insurance companies). However, the currently
available third-party information is not accurate enough
12. For a detailed proposal that would require the IRS to collect
additional tax payments linked to coverage status, see the
description of a retroactive coverage backstop in Christen L.
Young, ree Ways to Make Health Insurance Auto-Enrollment
Work (USC-Brookings Schaeer Initiative for Health Policy,
June 2019), www.brookings.edu/wp-content/uploads/2019/06/
Yonu_Autoenrollment_6.19.19.pdf (445 KB).
to adequately enforce such a policy.
13
Imposing new
taxes on the basis of coverage status—and collecting
those taxes—would require the IRS to obtain more accu-
rate and comprehensive data on insurance status than are
currently available through the information returns led
by third parties. e IRS could use that more accurate
data to verify the information that people report on their
tax returns. Legislation establishing the default coverage
policy could include additional reporting requirements
and provide funding for the IRS to improve its ability
to accurately measure the monthly coverage status of tax
lers, which would enhance the IRS’s ability to audit.
e IRS would only be able to verify the coverage status
of, and enforce the collection of tax payments from,
people who led income tax returns. Exempting people
whose income fell below the tax-ling threshold from the
tax obligations associated with default coverage would
facilitate enforcement. Exempting those people would
have a very small eect on the taxes collected because
they tend to have very low income and they would be
eligible for large premium subsidies to oset all or nearly
all of the tax obligation under all of the proposals that
CBO reviewed. (For tax year 2019, a single adult under
the age of 65did not have to le an income tax return
if his or her gross income was less than $12,200, which
was just over the eligibility threshold for a premium tax
credit. e legislation also could adjust the tax-ling
threshold.)
Under proposals in which the Medicaid and CHIP
programs continued to exist and provide default coverage
for people who were eligible for those programs—sim-
ilar to Approach 1—the IRS also would have to iden-
tify whether people were eligible for those programs to
determine whether they would be responsible for taxes
to nance the default plan. at would require collecting
information from state agencies or making a simplied
13. A recent study found that the number of people identied as not
having insurance using the currently available third-party reporting
(13 percent) was substantially higher than the number of people
estimated to not have insurance using nationally representative
survey data (9 percent to 10 percent). By contrast, the number
of people without coverage who self-reported being uninsured
on their tax returns (8 percent) was lower than the nationally
representative estimates. ose dierences indicate that currently
available third-party reporting to the IRS is insucient to verify
the self-reported information. See Ithai Z. Lurie and James Pearce,
Health Insurance Coverage From Administrative Tax Data, Oce
of Tax Analysis Working Paper 117 (Department of the Treasury,
February 2019), https://go.usa.gov/xGBZV (PDF, 18.49 KB).

18 Policies to Achieve NeAr-UNiversAl heAlth iNsUrANce coverAge october 2020
eligibility determination on the basis of the income and
age that tax lers reported on tax returns. It would be
challenging for the IRS to make accurate eligibility deter-
minations during the tax-ling process, because eligibil-
ity for Medicaid and CHIP is based on monthly income,
which may vary throughout the year, whereas the IRS
relies on annual income.
Amount of the New Taxes. Partially subsidized default
coverage could create a large new tax obligation for
people without an alternative source of coverage, partic-
ularly people with income that was too high to qualify
for premium subsidies. For example, if people with
income above 400percent of the FPL were not eligi-
ble for any subsidies other than for employment-based
coverage (as is the case under current law), the new
tax obligation for someone with an income just above
the eligibility threshold ($48,560 for a single person in
2019) would have been about $5,700 for a 40-year-old
if the cost of the default plan was similar to the cost of
the second-lowest-cost silver plan under current law in
2019.
14
at would have amounted to about 12per-
cent of income for someone with an income just above
400percent of the FPL and about 8percent of income
for someone with an income equal to 600percent of the
FPL.
ose amounts far exceed the maximum of 2.5percent
of income that was specied under the ACA as the pen-
alty for not having health insurance coverage before that
penalty was eliminated under the 2017tax act. However,
those people also would receive health insurance cover-
age through a default plan for the period in which they
did not have another source of coverage; that would not
be the case under systems using an individual mandate
penalty. As people became more familiar with such a pol-
icy over time, more people might elect to actively enroll
in a plan and pay premiums earlier in the year, which
would reduce the number of people responsible for large
tax payments at the time tax returns were led.
It could be dicult for the IRS to enforce the payment
of premium-equivalent taxes, particularly if those taxes
were large and exceeded the amount of the tax refund
that lers were owed otherwise. e IRS had limited
14. For estimates of average marketplace premiums, see Kaiser Family
Foundation, “Average Marketplace Premiums by Metal Tier,
2018–2020,” https://tinyurl.com/y2pzmu34.
authority to collect the individual mandate penalties
specied under the ACA. Legislation that enacted
partially subsidized default coverage could grant the IRS
greater authority to collect premium-equivalent taxes
by garnishing wages, imposing liens, or other means.
However, those strategies might be controversial.
Structuring Premium-Equivalent Taxes. e premium-
equivalent tax could be structured and collected in two
main ways, both of which would add reporting require-
ments and additional complexities to the tax system. e
simplest option would be to levy a tax directly on those
covered by the default plan. at would include people
who enrolled in the default plan on their own or through
a health care provider or who were enrolled by the
government automatically. It also would include people
whom the IRS determined did not have another source
of coverage for certain periods of the year. at option
would be more likely to result in large tax bills at the end
of the year for people covered by the default plan, unless
withholding was adjusted by those taxpayers during the
year to reect their lack of coverage and anticipated tax
obligation. Although income withholding amounts can
be changed, most workers do not routinely make adjust-
ments. People who actively enrolled in the default plan
during the year could begin making estimated tax pay-
ments when they enrolled. Alternatively, the IRS could
automatically withhold people’s estimated tax obligations
if their coverage status could not be veried.
Another option for collecting the new tax would be to
levy a premium-equivalent tax on all tax lers, including
people who were enrolled in coverage for the entire year.
People who demonstrated through third-party reporting
that they had qualifying health insurance would then be
able to fully oset that tax obligation with a tax credit of
equivalent size. Eorts could be made to allow insured
lers to adjust their withholding accordingly throughout
the year to anticipate the osetting tax credit. However,
because some people who were enrolled in employ-
ment-based insurance or other plans might not adjust
their withholding, this option probably would cause
some of those people to pay too much in taxes during
the year and then receive large tax refunds at the end of
the year when the IRS determined that they were eligible
for a fully osetting tax credit. is option would reduce
the number of people with a large tax obligation due at
the time of tax ling, but it also would be more complex
to administer.

19october 2020 Policies to Achieve NeAr-UNiversAl heAlth iNsUrANce coverAge
Determining Payments to Insurers When the Default
Plan Is Part of a Risk-Adjustment System. To ensure
that the premium-equivalent taxes for the default plan
were similar to equivalent plans that were available for
active enrollment, the default plan could be part of a
risk-adjustment system that included those plans. In a
risk-adjustment system, all plans in the system make
or receive payments that adjust their premiums for the
costliness of their enrollees relative to that of enrollees
in other plans in the system. In anticipation of receiving
or making those payments, plans in the risk-adjustment
system set their premiums in part to reect the cost of
covering all enrollees in the risk pool. (A risk pool refers
to a group of plans that share the cost of covering all
enrollees in the pool. ose costs are shared through a
risk-adjustment system.) Determining the appropriate
payments to compensate plans that are included in the
risk-adjustment system would require determining the
number of people covered by the default plan and the
expected cost to insure them relative to that of enrollees
in other plans.
Determining the Number of People Covered by the Default
Plan. One challenge would be estimating the number of
people who would be covered by the default plan. Two
groups would be covered by the default plan: people
who were enrolled in the plan and people whom the IRS
would need to identify as not having another source of
coverage. (People might enroll during the year on their
own or through a health care provider, or they might be
enrolled by the government automatically.) e people
who enrolled in the default plan during the year would
all be identied, but the IRS might have diculty iden-
tifying everyone else without another source of coverage
because of the gaps in reporting discussed earlier. In
addition, it would be even more dicult for the IRS to
identify the coverage status of people who did not le
tax returns because their income fell below the tax-ling
threshold. If the IRS underestimated the number of peo-
ple who did not have another source of coverage during
the year, the people who enrolled in the default plan
during the year (many of whom would do so only after
experiencing a costly episode of care) would represent a
larger share of the people who were identied as covered
by the default plan. e risk-adjustment payments to the
default plan would then have to be larger to reect the
higher average cost of the people who were identied as
being covered by the default plan relative to the entire
group of eligible people.
Setting Payments for Insurers Using a Risk-Adjustment
System. Once the government identied the group of
people who would be covered by the default plan, it
would determine the risk-adjustment payments for all
plans in the system on the basis of the expected health
care spending of people covered by the default plan and
other plans in the risk pool. To determine the size of the
payments, the government would start with a measure of
average spending for all people in the risk pool and then
adjust that average up or down to account for plans that
tended to have more or less costly enrollees than average.
ose calculations would be done using a new or
modied risk-adjustment system, but the ability of the
risk-adjustment system to predict the expected cost of
people covered by the default plan would be imperfect.
15
Under current law, the health insurance marketplaces use
a risk-adjustment system established by the ACA that
compensates insurers who attract a more costly group of
enrollees by transferring funds from insurers who attract
a less costly group of enrollees. at system adjusts
payments primarily on the basis of chronic conditions,
such as diabetes and hypertension. Such a risk-adjust-
ment system probably would not adequately compen-
sate insurers for the people who would be identied as
being covered by the default plan because their spending
would disproportionately include acute care events, such
as heart attacks and car accidents. Modications to the
risk-adjustment system would be required to adequately
capture the dierences in costs between people who
would be covered by the default plan and people who
would actively enroll in other plans. Risk scores for some
people who were eligible for default coverage would have
to be computed solely on the basis of their demographic
characteristics.
15. Existing risk-adjustment systems (such as those used in the
Medicare Advantage and Medicare Part D programs and the
nongroup market) do not entirely capture the cost of people
in the markets in which they are currently used. In particular,
some plans are able to receive larger risk-adjustment payments
because they record additional health conditions for their
enrollees. See Michael Geruso and Timothy Layton, “Upcoding:
Evidence From Medicare on Squishy Risk Adjustment,” Journal
of Political Economy, vol. 128, no. 3 (2020), pp. 984–1026,
http://doi.org/10.1086/704756. Research also shows that
insurers change their benet designs to attract enrollees who
result in risk-adjustment payments that are large relative to
their cost. See Colleen Carey, “Technological Change and Risk
Adjustment: Benet Design Incentives in Medicare Part D,”
American Economic Journal: Economic Policy, vol. 9, no. 1 (2017),
pp. 38–73, http://doi.org/10.1257/pol.20140171.

20 Policies to Achieve NeAr-UNiversAl heAlth iNsUrANce coverAge october 2020
Determining the appropriate risk-adjustment payments
also would depend on the overall risk pool that the
default plan was a part of—that is, the other plans that
participated in the risk-adjustment system. e default
plan could be part of the same risk pool as other plans
that are available for active enrollment, such as the
nongroup market under current law. e default plan
probably would draw a less costly group of people than
the current nongroup market because, on average, those
who do not enroll in coverage tend to spend less on
health care. If the IRS was able to accurately identify the
less-costly people who would be covered by the default
plan, then adding a default plan to the same risk pool
as the current nongroup market would probably reduce
overall premiums in that market.
Other Risk-Management Tools. e government also
might need to use other tools to compensate insur-
ers for the cost and nancial risk of administering the
default plan or for the cost of being part of the same
risk-adjustment system. Particularly in the initial years,
private insurers would be uncertain as to the number of
people who would be covered by the default plan and
their health care spending. As a result of that uncertainty,
private insurers might be less willing to participate in
a risk-adjustment system that included a default plan
or they would require higher premiums to take on the
additional risk of oering coverage in the initial years
of implementation. To mitigate those concerns, the
government could use other tools, such as a reinsurance
or risk-corridor program, to reduce uncertainty and
stabilize premiums for the default plan and other plans
in the risk pool in the initial years after the default plan
wasintroduced.
A reinsurance program would compensate all insurers
that participated in the same risk-adjustment system
(for example, all insurers in the nongroup market) if the
market as a whole experienced unanticipated higher costs
in the years following the introduction of the default
plan. A risk-corridor program would compensate partic-
ular plans (such as the default plan) if their actual costs
exceeded anticipated costs by a particular threshold.
Informing People About eir Eligibility for Default
Coverage and the Plan’s Benets. In order for the
default plan to provide comprehensive access to care to
otherwise uninsured people, those without an alternative
source of coverage would need to be made aware that
they were automatically covered by the default plan and
be informed of the plan’s benets. In the initial years fol-
lowing implementation of default coverage, an outreach
campaign could educate people about their eligibility for
the default plan and its associated benets. People would
need to know who would be covered by the default plan
automatically, what cost sharing would be required by
that plan, and which providers participated in the default
plan. An eective outreach campaign would increase the
number of people who would seek health care know-
ing that the cost of their care would be covered by the
default plan, but it would be dicult to fully inform
allpeople.
If only some providers participated in the default plan,
informing people about which providers were included
in the default plan’s network would be challenging
because, in many cases, those people would not have
previous experience using the default plan. If people
were not adequately informed, some would seek care
without knowing whether a provider was in or out of the
default plan’s network. If people received treatment from
a provider that did not participate in the network of the
default plan, they could encounter “surprise billing”—
that is, they could be required unexpectedly to pay for
the full cost of that care at the out-of-network rate (a
price that is typically much higher than the rate nego-
tiated by insurers for providers that participate in the
plan’s network).
Policy Approaches
CBO identied four general approaches that have
the potential to achieve near-universal coverage using
premium subsidies and automatic coverage through a
default plan that would be partially or fully subsidized.
e introduction of default coverage could be accom-
plished while otherwise preserving most features of the
current system or by completely overhauling the system.
e four approaches described here cover that spectrum;
each successive approach would require more signicant
changes.
Approach 1: Partially Subsidized Default Coverage
That Operates in Tandem With Current Sources of
Coverage
Policies based on this model would retain most key
features of the current system. Specically, employment-
based coverage would continue to play a large role,
income-based subsidized coverage would still be available
through existing health insurance marketplaces, and

21october 2020 Policies to Achieve NeAr-UNiversAl heAlth iNsUrANce coverAge
current eligibility criteria for Medicaid and CHIP would
be preserved.
e most signicant new feature of this approach relative
to current law would be the introduction of automatic
coverage through a partially subsidized default plan for
people who do not otherwise enroll in health insurance
and are not eligible for Medicaid or CHIP. To provide
subsidized default coverage to nearly all people who do
not enroll in another source of coverage, the employer
rewall also would be eliminated. (See Box 1 for a dis-
cussion of the challenges of providing default coverage
while retaining the employer rewall.) Full premium
subsidies would be extended to people whose income
is below 100 percent of the FPL. Policies based on this
approach could further reduce out-of-pocket premiums
and encourage active enrollment in coverage from other
sources by increasing the generosity of premium subsi-
dies for other income groups.
Default Coverage. For people who are ineligible for
Medicaid and CHIP and not enrolled in another source
of coverage, default coverage would be provided either by
a private plan or by a new public health insurance option
that would be oered through existing health insur-
ance marketplaces. Premium-equivalent taxes would be
collected from those otherwise uninsured people through
the tax system to help nance the default coverage and
maintain incentives for people to actively enroll in other
sources of insurance. ose taxes would be equal to
the premium of the default plan less any premium tax
credits for which the person was eligible (similar to the
amounts those people would pay to enroll in an equiva-
lent plan through the marketplaces) for each month the
person did not have another source of coverage. Lower-
income people would contribute less to the nancing of
default coverage, and people whose income fell below
the tax-ling threshold would not be required to pay any
premium-equivalent taxes. People who are currently eli-
gible for but not enrolled in Medicaid and CHIP would
receive default coverage through those programs (and no
premium-equivalent taxes would be collected).
Enrollment Process. e enrollment process for
Medicaid and CHIP, nongroup coverage, and other
sources of coverage would remain unchanged from
that in eect under current law. For people who did
not actively enroll in a plan during an open-enrollment
period, a default private or public plan (or Medicaid
and CHIP, for those who were eligible) would provide
coverage without the need for individuals to actively
enroll. To use the default plan to receive covered health
care, individuals who were uninsured could enroll in the
plan at any time themselves or through certain health
care providers.
Premiums. Under this approach, premiums for
nongroup coverage would continue to be subsidized
through premium tax credits for low- and middle-in-
come people who obtained coverage through the health
insurance marketplaces.
Premium Subsidies for Nongroup Coverage. Eligibility
for premium tax credits to purchase nongroup coverage
through the health insurance marketplaces would be
extended to those whose income is below 100percent of
the FPL, allowing them to purchase a plan at a zero net
premium and lling in the “coverage gap” for people in
states that have not expanded Medicaid under the ACA.
(Under current law, many adults who reside in states that
have not expanded Medicaid and whose income is below
100percent of the FPL have no options for subsidized
coverage because they are ineligible for both Medicaid
and premium subsidies for plans obtained through the
health insurance marketplaces. ose people are often
referred to as falling into a coverage gap.)
Eligibility for health insurance subsidies could be
extended to additional households by raising the eligi-
bility threshold for premium subsidies from 400per-
cent of the FPL to 500percent of the FPL, or higher.
Under current law, people whose income is just under
400percent of the FPL are eligible for subsidies that
limit their cost of purchasing a silver plan to 9.78per-
cent of their income, whereas people with income just
over 400percent of the FPL receive no subsidies. (In
2019, the eligibility threshold was $48,560 for a single
person and $100,400 for a family of four.) People who
are eligible for subsidies pay premiums that are based pri-
marily on their income. People who are not eligible for
subsidies pay premiums that primarily depend on their
age, and those premiums are smaller for younger people.
e eect on premium payments of having income just
below or above the eligibility threshold is correspond-
ingly small for younger people and much larger for older
people. For example, 27-year-old single adults paid about
9 percent of their income, on average, for the lowest-cost
silver plan in 2019 if their income was $45,000 (eligible
for a subsidy) or $50,000 (not eligible). Sixty-year-old
single adults paid, on average, about 8 percent of their

22 Policies to Achieve NeAr-UNiversAl heAlth iNsUrANce coverAge october 2020
Box 1.
Introducing Default Coverage While Maintaining an Employer Firewall: Implications and Challenges
Under current law, people with an oer of aordable
employment-based coverage are ineligible for premium subsi-
dies in the health insurance marketplaces because of a provi-
sion of the Aordable Care Act known as the employer firewall.
In 2020, an oer of aordable employment-based coverage
is defined by the Internal Revenue Service as one in which an
employee’s out-of-pocket premium is less than 9.78percent of
household income for a single plan. The employer firewall was
enacted as a way to minimize reductions in employment-based
insurance by preventing people with an oer of aordable
employment-based coverage from switching to subsidized
coverage in the marketplaces and to encourage employers to
continue oering such coverage.
Although introducing default coverage while maintaining an
employer firewall is possible, the Congressional Budget Oce
did not find any detailed policy proposals that would achieve
near-universal coverage while maintaining the firewall. Main-
taining an employer firewall would present several challenges.
Those challenges would arise only for proposals in which
default coverage was partially subsidized. An employer firewall
would not be relevant for proposals in which default coverage
was fully subsidized through broad-based tax revenues.
The key implications of introducing default coverage while
maintaining the employer firewall, compared with approaches
that would remove the firewall, are as follows:
■ Fewer changes would be made to people’s sources of
coverage under current law, depending on the relative
generosity of the subsidy for default coverage and other
sources of coverage.
■ Fewer gains in coverage would occur if people with an
oer of aordable employment-based insurance were not
required to enroll in default coverage. If those people were
eligible for default coverage and responsible for the asso-
ciated tax payment, the firewall would prevent them from
being eligible for subsidies to oset the tax obligation, and
they would be liable for a large tax payment.
■ Administrative complexity would be greater because a
government entity would have to verify whether each unin-
sured person had an oer of aordable employment-based
coverage.
Fewer Changes to Sources of Coverage
Under proposals that introduced default coverage and retained
the employer firewall, there probably would be fewer changes
to current sources of coverage than under the approaches
described in this report that would remove the firewall. That
is, more people with employment-based insurance probably
would retain that coverage if the firewall remainedintact.
The extent of changes to sources of coverage would depend
on the relative generosity of the subsidy for default cover-
age and other sources of coverage, the size of the firm, and
the income distribution of employees eligible for an oer
of employment-based coverage. If the subsidy available for
default and other sources of coverage was the same as the
premium tax credits under current law, employers’ incentives
to oer coverage most likely would be similar to the incentives
that exist under current law. However, if subsidies became
more generous and enough employees found subsidized
default and other coverage to be a more attractive alternative
to employment-based coverage, some employers might have
fewer incentives to oer coverage.
Fewer Gains in Coverage If People With an Oer
of Aordable Employment-Based Insurance Were
Ineligible for Default Coverage
A policy that introduced partially subsidized default coverage
while maintaining the employer firewall would need to specify
whether people with an oer of aordable employment-based
coverage who chose not enroll in their employer’s plan (or an
alternative plan) would be required to enroll in default cover-
age and responsible for the associated premium-equivalent
tax to finance that coverage. If those people were eligible for
default coverage and responsible for paying the associated
tax, the firewall would prevent them from being eligible for
subsidies (such as premium tax credits) to oset the tax obliga-
tion. Those people would then be liable for a large tax, which
could be surprising and particularly burdensome for people
with modest income.
A proposal could include additional requirements to minimize
the number of people who would be covered by the default
plan and responsible for large tax payments. For example,
the policy could require employers to automatically enroll
all of their employees in their least expensive plan during
the open-enrollment period unless the employee chose an
alternative plan oered by the employer, provided proof of
Continued

23october 2020 Policies to Achieve NeAr-UNiversAl heAlth iNsUrANce coverAge
income if that income was was $45,000 and 23 percent
if their income was $50,000.
16
Extending eligibility
to households whose income is up to 500 percent or
more of the FPL would eliminate any sharp increases
in premiums for people in that income range, but older
people just above the new eligibility threshold might face
a similar sharp increase.
Premium subsidies could be made more generous by
decreasing the aordability thresholds (the percentage
of income that people who qualify for subsidies are
expected to pay for a benchmark plan) or by benchmark-
ing the subsidy level to a more generous plan—for exam-
ple, to the second-lowest-cost gold plan rather than the
second-lowest-cost silver plan. More generous subsidies
would both reduce the amount that people would pay
to enroll in nongroup plans and reduce the size of the
premium-equivalent tax that would be levied on people
if they did not enroll in a plan. But larger subsidies also
would increase the cost to the government.
Gross Premiums in the Nongroup Market. Gross premi-
ums (the total premium charged by insurers before any
16. See Figure 2 in Rachel Fehr and others, How Aordable Are
2019 ACA Premiums for Middle-Income People? (Kaiser Family
Foundation, March 2019), https://tinyurl.com/y2lvvmkh.
premium subsidies are applied) in the nongroup market
probably would decrease because previously uninsured
and less costly individuals would be brought into the risk
pool through default coverage.
If the approach included a new public option, premi-
ums could be even lower. e public option could have
lower premiums than comparable private plans available
through the health insurance marketplaces if the pub-
lic option had lower costs—because of lower provider
payment rates or administrative costs, for example. Gross
premiums in the marketplaces also might decrease if the
public option put downward pressure on the premiums
of private plans. Alternatively, the public option could
have higher premiums if it operated less eciently, used
fewer managed care tools that constrained utilization
(such as prior authorization or gatekeeping), or attracted
enrollees who were less healthy in ways that were not
captured by the risk-adjustment system. A public option
with higher premiums also could have a broader network
of participating providers or higher payment rates, which
would make care more accessible.
In addition, some low- and middle-income people who
previously obtained coverage through their employ-
ers would be brought into the nongroup market once
they were eligible for premium subsidies—because of
other coverage, or opted out. (A requirement that certain
large employers with more than 200employees auto-enroll
those employees in a health insurance plan was attempted in
the past, but that requirement was not implemented and was
repealed by Bipartisan Budget Act of 2015before it took eect.
Some of the concerns related to employer auto-enrollment
include how to determine whether an employee already has
coverage through a family member or dependent and how
much discretion employers have in choosing a health insurance
plan for their employees.)
Alternatively, if a proposal prevented people with an oer of
aordable employment-based coverage from receiving default
coverage and it did not levy the associated tax to finance
default coverage, such a proposal would result in fewer gains
in coverage. In that case, many uninsured people who do not
currently take up their oer of aordable employment-based
coverage (or another source) would probably continue to
decline such coverage, leaving millions of people without
health insurance.
Increased Administrative Complexity
Maintaining an employer firewall alongside default coverage
would increase the administrative complexity and cost of
implementing default coverage. Those administrative complex-
ities and costs would arise because a government entity would
have to verify whether each uninsured person had an oer of
aordable employment-based coverage, which could require
developing new reporting systems. The eectiveness of the
employer firewall also would depend on how strongly it was
enforced—proposals that increased the relative generosity of
the subsidy for default and other coverage would increase the
need to enforce compliance with the employer firewall.
Box 1 . Continued
Introducing Default Coverage While Maintaining an Employer Firewall: Implications and Challenges

24 Policies to Achieve NeAr-UNiversAl heAlth iNsUrANce coverAge october 2020
the elimination of the rewall—which could increase
or decrease gross premiums, depending on the average
spending of those enrollees.
Net Premiums in the Nongroup Market. ose lower gross
premiums in the nongroup market would primarily
decrease net premiums (the premiums paid by individ-
uals after any premium subsidies are applied) for unsub-
sidized, higher-income households because net premi-
ums for subsidized households are already capped as a
percentage of their income. Net premiums for low- and
middle-income subsidized households could decrease if
the policy increased the generosity of premium subsidies
in the ways discussed earlier. Net premiums also would
fall to zero for low-income households that became
newly eligible for premium subsidies because they were
living in a state that had not expanded Medicaid.
Premiums for Other Types of Insurance. Premiums for
employment-based insurance would continue to be
subsidized through existing tax preferences. Premiums
for some employment-based plans might change,
depending on whether the people who switched from
employment-based coverage to subsidized marketplace
coverage were more or less healthy than the people who
retained employment-based coverage. Premiums for
people obtaining coverage through other sources (such as
CHIP) would remain about the same.
Cost Sharing and Benets. Cost sharing for existing
sources of coverage could remain unchanged from cur-
rent law under some specications, or it could decrease.
For example, cost sharing could decrease for some groups
if eligibility for cost-sharing reductions was expanded,
or if premium subsidies were benchmarked to a more
generous plan, such as a gold plan. Covered benets for
existing sources of coverage would remain unchanged
from current law. e default private or public plan
could be required to have the same amount of cost shar-
ing as the benchmark plan used to determine premium
subsidies (currently a silver plan, with income-based
CSRs) or a less generous plan.
Role of Private Plans. Private plans would continue to
play a large role under this approach. Most people under
the age of 65 would continue to receive private cover-
age either through employers or through the nongroup
market. Enrollment in nongroup private plans would
increase if default coverage was provided by a private
plan. People who were newly eligible for subsidized
coverage through the marketplaces would enroll in
private plans, and some people would gain coverage
through a private default plan.
Even if the approach included a public option, private
plans would still continue to play a large role. Most peo-
ple under the age of 65 would continue to receive private
coverage through employers or in the nongroup market.
Enrollment in nongroup private plans could increase or
decrease: On the one hand, some people would switch
from private coverage to the new public option; on
the other hand, the total size of the nongroup market
would increase as more people whose income fell below
100percent of the FPL became eligible for premium
subsidies and as some low- and middle-income workers
switched from employment-based coverage to a subsi-
dized marketplace plan.
Role of Employment-Based Coverage. Employment-
based coverage would play a smaller role under this
approach than under current law, but most people who
currently obtain coverage through employers probably
would continue to do so, in part because of its tax advan-
tages. Employment-based insurance also would continue
because of its eectiveness in pooling risks and because
of the lower costs for some administrative activities (for
instance, for marketing and collecting premiums) com-
pared with nongroup insurance.
Eliminating the employer rewall would lead some
low- and middle-income people who are eligible for
employment-based coverage to forgo that coverage in
favor of subsidized marketplace or default coverage.
Lower-income workers who were eligible for the largest
premium subsidies would be the most likely to choose
marketplace coverage over employment-based coverage,
and some rms would design their insurance oerings to
encourage them to do so. For example, some rms might
increase employees’ premium contributions to a level
that would make it more expensive for their lower-in-
come workers to purchase the employment-based plan
rather than purchase subsidized marketplace coverage.
Number of Employers Oering Insurance. Employers
would respond dierently to the elimination of the
rewall, depending on the income mix of their workers
and the number of workers in their rm. Employers with
workers whose income was too high to qualify for mar-
ketplace subsidies would have a strong incentive to oer
insurance even in the absence of the rewall. Employers

25october 2020 Policies to Achieve NeAr-UNiversAl heAlth iNsUrANce coverAge
with only some workers who were eligible for such subsi-
dies would weigh the costs and benets to their employ-
ees of oering insurance. ose employers also would
consider what fraction of their employees would be likely
to take up that oer, because insurers often charge higher
premiums to small rms that do not have high participa-
tion rates among their workers. Small rms with many
workers who qualied for subsidies would be the most
likely to stop oering coverage if removing the rewall
caused those workers to switch to subsidized marketplace
coverage.
Altogether, employers probably would have fewer incen-
tives to oer coverage once the employer rewall was
eliminated, but the number of employers that changed
their oerings would depend on the generosity of the
premium subsidies available to their workers. If the
generosity of premium subsidies for marketplace plans
remained unchanged from current law, the number of
employers who stopped oering insurance would proba-
bly be small. Some employers might not oer coverage if
enough of their employees found subsidized marketplace
and default coverage to be a more attractive alternative
than employment-based coverage. In that case, employ-
ers generally would oset that reduction in health bene-
ts by oering higher wages to their employees.
However, eliminating the employer rewall might lead
a few additional employers to oer coverage. Currently,
some rms may choose not to oer coverage because if
they did so, the rewall would prevent their low- and
middle-income employees from enrolling in more attrac-
tive subsidized marketplace coverage. If the rewall was
eliminated, those rms could oer coverage primarily for
the benet of higher-income employees, who would not
qualify for subsidies, without preventing their low- and
middle-income employees from being eligible for sub-
sidized marketplace or default coverage. Because enroll-
ment in that employment-based coverage would largely
be limited to higher-income employees, those rms’ total
costs of oering coverage would be lower in the absence
of the rewall.
Although eliminating the rewall might lead slightly
more rms to oer employment-based coverage, over-
all enrollment in that coverage probably would decline
because the number of low- and middle-income
employees switching to marketplace or default coverage
probably would exceed the number of higher-income
employees enrolling in newly oered employment-based
coverage.
Role of Public Programs. Under this approach, existing
public programs would play a role similar to the role
they play under current law. Many low-income people
would continue to receive coverage through Medicaid
or CHIP, and some would continue to use other public
coverage, such as Medicare for the disabled.
Along with extending eligibility for marketplace sub-
sidies to people whose income was below 100percent
of the FPL, the federal government would nance the
entire cost of the expansion population in states that
expanded Medicaid under the terms of the ACA (rather
than 90percent of the costs as under current law).
at would give state policymakers exibility to choose
whether to provide subsidized coverage to people below
100percent of the FPL through Medicaid or market-
place plans. Because both forms of coverage would be
fully subsidized by the federal government, states that
have already expanded Medicaid under the terms of
the ACA would not have a nancial incentive to scale
back their expansion of the program. Other states could
choose to expand Medicaid (with the federal government
nancing the entire cost) or they could cover those peo-
ple through marketplace subsidies, depending on their
priorities. Fully nancing the cost of Medicaid enrollees
made eligible through expansion under the terms of the
ACA would increase costs incurred by the federal govern-
ment for covering those people.
Public plans would play a larger role if the approach
included a new public option that was oered through
health insurance marketplaces and that provided default
coverage. More people would be enrolled in public
coverage through the new public option, but enrollment
in the public option would be a small share of overall
enrollment because most people who currently obtain
private insurance through employers would continue to
do so, and some people in the nongroup market would
continue to choose private plans.
Variants and Examples of is Approach. Covering all
people without an alternative source of coverage with
a default plan could be accomplished in dierent ways
by dening what type of entity would provide default
coverage. Variants of this approach include a default plan
that would be provided by private insurers or through a

26 Policies to Achieve NeAr-UNiversAl heAlth iNsUrANce coverAge october 2020
public option that also would be available to all people
through existing health care marketplaces.
Private Default Coverage. Under this variant, a private
plan could serve as default coverage for people who did
not enroll in another plan or program. A proposal by
Fiedler and others incorporates all of the key features
of this approach, including a similar default coverage
mechanism and the expansion of eligibility for subsi-
dized coverage, but it does so in ways that are somewhat
dierent from those described here.
17
For example,
rather than extending eligibility for marketplace subsi-
dies to those whose income was below 100percent of
the FPL, the proposal would provide states that have not
expanded Medicaid incentives to do so. at proposal
has the potential to achieve near-universal coverage if all
states chose to expand Medicaid when faced with those
incentives.
Public Option Oered rough the Marketplaces. A
public option that was oered through the existing
health insurance marketplaces could provide near-uni-
versal coverage if the option acted as a default plan and
provided coverage to all otherwise uninsured people.
e public option could be specied to have the same
generosity as the benchmark plan used to determine the
amount of premium subsidies (currently, a silver plan),
with comparable income-based cost-sharing-reduction
subsidies. People who were assigned to the public option
through the default mechanism would be responsible for
tax payments that were equal to the net premium they
would have faced had they enrolled through the health
insurance marketplaces.
Another proposal, by Blumberg and others, would incor-
porate all of the key features of this approach, including
introducing a public option with a similar default role
and expanding eligibility for subsidized coverage.
18
at proposal also would increase the generosity of
17. See Matthew Fiedler and others, “Building on the ACA to
Achieve Universal Coverage,” New England Journal of Medicine,
vol. 380, no. 18 (May 2, 2019), pp. 1685–1688, http://
doi.org/10.1056/NEJMp1901532.
18. See “Simulated Reform Packages: Reform 5,” in Linda J.
Blumberg and others, From Incremental to Comprehensive Health
Insurance Reform: How Various Options Compare on Coverage and
Costs (Urban Institute, October 2019), p. 6, https://tinyurl.com/
yy9atuf7 (PDF, 1.05 MB).
marketplace subsidies and establish a federal reinsurance
program for the nongroup market. Many other proposals
would introduce a public option in the nongroup mar-
ket, but they would not achieve near-universal coverage
unless paired with a default coverage mechanism.
19
Approach 2: Partially Subsidized Default Coverage
Through a Large Public Program That Replaces
Medicaid, CHIP, and the Nongroup Market and
Retains Employment-Based Coverage
Under this approach, a new public health insurance
program would replace the current nongroup market and
Medicaid and CHIP acute care coverage, and all coverage
would be provided through employers, the new public
program, or existing public programs such as TRICARE.
e public program would allow people to choose
between a publicly administered plan and multiple
privately administered plans meeting the same minimum
requirements for cost sharing and covered benets. at
structure would be similar to that of the Medicare pro-
gram, which allows beneciaries to choose between the
publicly administered Medicare fee-for-service program
and private Medicare Advantage plans. e publicly
administered plan would serve as the default plan, which
would provide automatic coverage for people who did
not have an alternative source of coverage.
Large employers would be required to oer coverage that
qualied for the same tax preferences that are available
under current law or to make mandatory contributions
to the public program. Employees could choose to
receive coverage through their employer or the public
program. All low- and middle-income people, includ-
ing those with an oer of employment-based coverage,
would be eligible for premium subsidies to purchase
coverage through the public program.
Enrollment Process. Enrollment in the public pro-
gram could occur through an online portal or an alter-
native process administered by one or more federal
or state agencies, whereas the enrollment process for
employment-based coverage and other sources of cov-
erage would remain unchanged from the processes used
19. See the Keeping Health Insurance Aordable Act of 2019, S. 3,
116th Cong.; the Choose Medicare Act, H.R.2463 and S. 1261,
116th Cong.; the Medicare-X Choice Act of 2019, H.R. 2000
and S. 981, 116th Cong.; and the CHOICE Act, H.R. 2085 and
S. 1033, 116th Cong.

27october 2020 Policies to Achieve NeAr-UNiversAl heAlth iNsUrANce coverAge
under current law. For people who did not actively enroll
in a plan, the public plan would provide default coverage
without the need for active enrollment.
Premiums. Premiums in the new public program could
be regulated in a manner similar to that governing the
nongroup market under current law (which stipulates
that premiums can vary by age, family size, geography,
and tobacco use). Alternatively, they might be allowed
to vary on the basis of a more limited set of factors (such
as requiring that a plan charge the same premium to all
people within the same geographic area). ose choices
would aect both the gross premiums under the new
program and the net premiums that dierent people
would face after applying any relevant premium subsi-
dies. As under current law, premium subsidies would be
based on the percentage of income that people would be
required to pay to purchase a benchmark plan.
Gross Premiums in the Public Program. Gross premiums in
the public program would depend on the average health
care spending of people who were enrolled in the pro-
gram, which might be dierent from the average spend-
ing of people enrolled in nongroup plans under propos-
als similar to Approach 1(whether or not a public option
was oered). In addition to covering people currently
enrolled in marketplace plans and other nongroup insur-
ance plans, the public program would cover people who
are currently uninsured (who tend to be younger and
healthier), those who are currently enrolled in Medicaid
and CHIP (who tend to be less healthy), and some
people who are currently enrolled in employment-based
plans (who could be more or less healthy, depending on
the generosity of the public program and how employers
adjusted their coverage oerings in response to the new
policy).
Net Premiums in the Public Program. If premiums in the
new program were regulated in a manner similar to that
governing the nongroup market under current law, net
premiums in the proposed public program would be
lower than in the nongroup market (as it operates under
current law) for the low- and middle-income people
who were eligible for subsidies. People with low income
would receive a subsidy that would cover the full cost of
the benchmark plan used to determine subsidies in the
new public program. Middle-income people would be
eligible for more generous premium subsidies than the
ones that are available through the health insurance mar-
ketplaces under current law. As with Approach1, people
who received coverage through the default mechanism
would have a net tax liability equal to the income-based
premiums they would have paid if they had actively
enrolled in the public plan. Higher-income people who
enrolled in the new public program and were not eligible
for subsidies would face the entire gross premium of
plans in the program.
Premiums for Employment-Based Insurance. Premiums
for employment-based coverage also might change if
the public program attracted a large number of people
who currently are enrolled in employment-based plans,
and if the risk prole of those remaining in employ-
ment-based coverage diered from that existing under
current law. For example, if the public program attracted
less healthy individuals (who tend to be more costly to
insure), premiums could decrease for those remaining in
employment-based coverage.
Cost Sharing and Benets. Plans in the public pro-
gram would be required to have a minimum generosity
level. For example, they could be required to have the
same generosity as a silver or gold plan, with income-
based cost-sharing requirements. As is the case with
cost-sharing reductions in the marketplaces under cur-
rent law, lower-income individuals would be responsible
for smaller cost-sharing payments. Depending on the
specications of the benet design, cost sharing could
remain unchanged from current law, or it could decrease.
For example, cost sharing could decrease for some groups
if income-based cost sharing was more generous than
under current law or if the minimum plan generosity
required by the public program was specied to be
greater than under current law.
Covered benets could be specied to include the
essential health benets required in the marketplaces
under current law, or they could be expanded to include
additional services, such as dental and vision coverage
and long-term services and supports. (Long-term services
and supports consist of health care and related services
provided to people with functional or cognitive limita-
tions to help them perform routine daily activities over
an extended period).
Role of Private Plans. Private plans would continue
to play a large role in both the new public program
and employment-based insurance. Some people under
the age of 65 would continue to receive private cov-
erage through their employers, but enrollment in

28 Policies to Achieve NeAr-UNiversAl heAlth iNsUrANce coverAge october 2020
employment-based insurance would decrease as some
workers and their families enrolled in the new public
program. e extent to which people shifted to the pub-
lic program would depend on the generosity of premium
subsidies, the generosity of coverage under the program
(that is, the actuarial value and covered benets) rela-
tive to employment-based coverage, and the size of the
required employer contributions and any other require-
ments or penalties to continue oering coverage.
Role of Employment-Based Coverage. Employment-
based coverage would continue, but it would play a
smaller role under this approach than under current
law. Large employers would be required to oer private
coverage or to oer coverage through the public pro-
gram by making mandatory contributions on behalf of
their employees (in which case employees could choose
between private plans and the public plan oered
through the public program). ose mandatory contri-
butions would be larger than the penalties employers
face for not oering coverage under current law. e
ability of employers to make contributions toward plans
oered through the public program would resemble
the nal rule governing recent health reimbursement
arrangements in eect under current law; that rule allows
employers to direct a limited amount of pretax premium
contributions to subsidize their employees’ choice of
private plans oered in the nongroup market.
20
Many large employers probably would continue oering
coverage outside of the public program, particularly if
the cost of oering that coverage was less than the contri-
butions they would be required to make to oer cover-
age through the public program; but the incentives for
employers to continue oering coverage would depend
on various features of the policy. For example, if the
mandatory contributions were structured as a percentage
of the employer’s payroll, rms employing higher-income
workers probably would nd it less expensive to continue
oering coverage outside of the public program. If the
policy did not include suciently large employer penal-
ties or requirements to oer coverage, employers would
have less incentive to oer coverage outside of the public
program.
20. For further discussion of the nal rule for health reimbursement
arrangements, see Katie Keith, “Final Rule on Health Reimbursement
Arrangements Could Shake Up Markets,” Health Aairs Blog
(June14, 2019), https://tinyurl.com/y6re7gdt.
A more generous level of benets and premium subsidies
for plans oered through the public program also would
make covering employees through the public program
more attractive than oering coverage outside of the
program. Although many employers would continue
to oer coverage, others would discontinue coverage
and their employees would receive coverage through
the public program. Some people, particularly those in
lower-income households who would have low or no
premiums for the public program, would opt for the
public program over employment-based coverage even
if their employer oered coverage. As a result, people
who retained employment-based coverage would have
higher income, on average, than the people enrolled in
employment-based coverage under current law and than
participants in the public program would have under this
approach.
Role of Public Programs. Enrollment in public coverage
would increase relative to current law. Although many
people would enroll in the public plan through the new
public program, many others would select a private plan
through the new program or through their employers.
e new public program could be based on an existing
program, such as Medicare, or it could be an entirely
new program. Some individuals would continue to use
other public coverage, such as the coverage Medicare
provides for the disabled.
Examples of is Approach. e Medicare for America
Act of 2019(H.R. 2452) uses a model that is similar to
the one described in this approach. at bill incorpo-
rates all of the key features of this approach, including a
new large public program called Medicare for America
that would entirely replace Medicaid, CHIP, and the
nongroup market.
21
It also includes requirements for
large employers and other elements that ensure many
people would continue to use private employment-based
coverage.
However, H.R. 2452 oers more specic details than the
general approach described here, and it includes some
elements that are dierent. For example, H.R. 2452also
would eliminate the existing Medicare program, and
it would cover those people in the new Medicare for
21. See the Medicare for America Act of 2019, H.R. 2452, 116th
Cong. For a related proposal, see Center for American Progress
Health Policy Team, Medicare Extra: Universal Coverage for Less
an $3 Trillion and Lower Health Care Costs for All (July 2019),
https://tinyurl.com/yyx9f55d (PDF, 1.18 MB).

29october 2020 Policies to Achieve NeAr-UNiversAl heAlth iNsUrANce coverAge
America program, which would allow them to choose
either a publicly administered plan or one of multiple
participating private plans. Large employers would pay
an 8percent payroll tax to help nance the new public
program if they did not oer coverage.
If enacted, the legislation would require the govern-
ment to auto-enroll all uninsured people in Medicare
for America. In CBO’s assessment, however, prospective
auto-enrollment of all uninsured people would not be
feasible because it would require the government to
identify every person at the moment they lost other
coverage and to begin collecting premiums from them.
e legislation has the potential to achieve near-universal
coverage if the public program also served as a default
plan that provided automatic coverage to uninsured
people who could not be auto-enrolled.
A dierent proposal by Blumberg and others also shares
the key features of this approach, including a new regu-
lated marketplace of private plans and a public plan that
would replace the current nongroup market, Medicaid,
and CHIP; generous subsidies to purchase insurance
through that marketplace; a continued role for employ-
ment-based coverage; and default coverage through a
public plan.
22
However, that proposal would not require
large employers to oer coverage or make mandatory
contributions.
Approach 3: Premium Subsidies for All People and
Default Coverage Through a Fully Subsidized Plan
e dening feature of this approach (often called a
premium support system) is that all people in the eligible
population under the age of 65 would receive a premium
subsidy from the government that was large enough to
cover the entire cost of a benchmark plan. Under this
approach, a specied level of benets would be provided,
along with cost-sharing reductions for low-income
people. People would use the subsidy to purchase a plan
of their choice from a health insurance marketplace that
included multiple private plans and, potentially, a public
option. Under this approach, preferential tax treatment
22. at proposal refers to default coverage as continuous
autoenrollment with retroactive enforcement. See “Description
of Policy Options: e Building Blocks of Healthy America,”
Variant 3: “HA With CARE,” in Linda J. Blumberg and others,
e Healthy America Program, An Update and Additional Options
(Urban Institute, September 2019), p. 3, https://tinyurl.com/
y3x3zyrs (PDF, 533 KB).
for employment-based health insurance would be elim-
inated. Employers would have little incentive to oer
primary health insurance coverage, but they might oer
supplemental coverage to reduce cost sharing or provide
additional benets not covered by marketplace plans.
e subsidies could be provided as a refundable tax
credit, which would reduce revenues and increase out-
lays, or as direct payments, which would only increase
outlays; the two would be economically equivalent.
23
Dierent variants could specify a less generous level of
benets (for instance, catastrophic coverage only) that
would be similar to those available through a bronze
plan under current law. Alternatively, the variants could
specify a more generous level of benets that would be
similar to those available through Medicare or a gold
plan.
is approach would represent a signicant change from
the current system: Employment-based insurance would
have a much smaller role than under current law, and
Medicaid and CHIP would no longer provide primary
coverage for acute care services, which include compre-
hensive major medical services and prescription drugs.
e Medicare program would continue to exist for peo-
ple over the age of 65 and the disabled population.
A fully subsidized benchmark plan would provide default
coverage for people who did not actively enroll in a plan
and would require no additional tax payments. Because
no additional tax payments for default coverage would
need to be collected from uninsured people, default
coverage would be substantially easier to implement than
would be the case with Approaches 1 and 2.
23. For example, under President George H.W. Bush’s 1992
proposal, low- and middle-income individuals who were
not covered by Medicare, Medicaid, the Veterans Health
Administration, or the Civilian Health and Medical Program of
the Uniformed Services would have been eligible for a tax credit
or tax deduction to purchase health insurance. e tax credit
would have extended up to a certain threshold based on modied
adjusted gross income and then it would have been phased out.
Such a proposal paired with the additional elements of default
coverage or a large and enforced individual mandate penalty
could achieve near-universal coverage. See R. Glenn Hubbard,
“e President’s 1992 Health Care White Paper: An Economic
Perspective,” National Tax Journal, vol. 45 no. 3 (1992), pp.
347–356, https://ntanet.org/NTJ/45/3/ntj-v45n03p347-56-
president-1992-health-care.html.

30 Policies to Achieve NeAr-UNiversAl heAlth iNsUrANce coverAge october 2020
Enrollment Process. People would use the premium sub-
sidy to purchase a plan from a health insurance market-
place. ey would be able to select a new plan each year
during an open-enrollment period.
24
For people who did
not actively enroll in a plan, a default zero-premium plan
would provide coverage without the need for them to
actively enroll.
Premiums. A premium subsidy that was equal to the full
premium of a specied benchmark plan in the market-
place would be more equitable if it varied with both
age and income instead of just with income.
25
People
who chose the benchmark plan (or a plan that cost less
than the benchmark plan) could enroll without paying
a premium. ey could still choose to enroll in a more
expensive plan, which would cover additional benets or
have lower cost sharing, but they would be responsible
for any additional costs above the benchmark subsidy.
e premium subsidy could be made more or less gener-
ous by adjusting the plan to which it was benchmarked.
Cost Sharing and Benets. e premium subsidy would
be large enough to cover the entire cost of a benchmark
plan with a minimum level of cost-sharing and covered
benets. e minimum amount of cost sharing could be
relatively high, as in a plan that provided only basic cat-
astrophic coverage for high-cost medical events in excess
of a certain dollar amount, or it could be relatively low,
similar to that of a gold plan available through the cur-
rent health insurance marketplaces. Cost-sharing reduc-
tions also would be available for certain populations,
such as low-income people. People without cost-sharing
reductions could choose to enroll in a plan with lower
cost-sharing amounts.
24. Some people also would be eligible to switch plans during a
special enrollment period if they experienced a qualifying life
event, such as the birth of a child.
25. If the 3:1 age-rating rule in eect under current law remained
in place and the refundable tax credit or direct payment did not
vary with age, the level of benets that could be purchased with
the refundable tax credit or direct payment amounts would vary
by age—for instance, a 64-year-old person would be able to
buy a much less generous plan than a 21-year-old. e amount
of benets that could be purchased with a refundable at tax
credit or direct payment also would vary by geographic area
because premiums vary by geographic area and state. For further
discussion of at premium tax credits, see American Academy
of Actuaries, “Auto-Enrollment Into Individual Market Health
Insurance Coverage” (September 2018), https://tinyurl.com/
y5a3v6yo (PDF, 215 KB).
e required covered benets under a premium support
system could be similar to the essential health bene-
ts specied by the ACA or the benets provided by
Medicare, or they could be based on something else,
such as a cost-eectiveness criterion. ey could include
additional benets, such as dental and vision services.
Role of Private Plans. Private plans would continue to
play a signicant role under this approach. People under
the age of 65could use the premium subsidy to purchase
a private plan from a marketplace; otherwise, they would
be covered under a zero-premium default plan.
Role of Employment-Based Insurance. Employers prob-
ably would have little incentive to oer primary health
insurance coverage under a premium support system if
everyone in the eligible population received a premium
subsidy from the government to purchase coverage
through a marketplace. However, depending on the pre-
mium subsidy amount, cost-sharing requirements, and
the type of benets oered by the marketplace plans, this
approach could allow employers to oer supplemental
coverage to their employees. Such supplemental cover-
age could be used to reduce cost-sharing amounts, or it
could be used to oer benets that were not available
through marketplace plans, such as dental and vision ser-
vices. If a marketplace plan provided basic catastrophic
coverage, for example, then employers could oer cov-
erage that provided the same benets they would have
provided under current law on top of the catastrophic
coverage. In such a case, their employees would experi-
ence little change in health insurance benets under this
approach compared with current law.
Because tax preferences for employment-based health
insurance would be eliminated under this approach,
people with the same income and similar family respon-
sibilities would receive the same benets for medical
costs, and subsidies would not be larger in higher tax
brackets. (Current law results in larger subsidies for peo-
ple in higher tax brackets because of the structure of tax
preferences for employment-based coverage).
Role of Public Programs. A premium support system
could include a public option that would be available
along with private plans in the new marketplace. As in
Approach 1, the public option could be modeled on an
existing public program, such as Medicare. A premium
support system also would need to specify the role of
other public programs, such as Medicaid, TRICARE, and
the Veterans Health Administration. Some components

31october 2020 Policies to Achieve NeAr-UNiversAl heAlth iNsUrANce coverAge
of those programs could continue to operate or provide
benets for services not covered by the premium support
system. e Medicaid and CHIP programs would be
substantially smaller because they would no longer pro-
vide primary coverage for acute care services. But those
programs could continue to provide long-term services
and supports for low-income and disabled populations.
Variants and Examples of is Approach. An approach
that oered everyone a subsidy covering the entire cost
of a benchmark plan that would be purchased through
a marketplace would depend on the way the bench-
mark plan was dened and how the marketplace was
structured.
Fully Subsidized Catastrophic Coverage for All. One
variant would be to benchmark premium subsidies to a
catastrophic plan with high levels of rst-dollar cost shar-
ing, such as a high-deductible plan.
26
However, under
the catastrophic plan, there would be no cost sharing for
the treatment of chronic conditions and preventive ser-
vices, such as vaccinations and prenatal care. Deductibles
would vary on the basis of household income, and indi-
viduals whose income was below a certain level would
not have a deductible. People could use their subsidy to
enroll in a catastrophic plan at no cost or they could use
their subsidy toward the cost of a more generous plan
oered through a marketplace of private plans if they
paid the additional premium. Under this variant, there
also could be a public option in the marketplace. Various
analysts have proposed an approach similar to the one
described here.
27
Fully Subsidized Generous Coverage for All. Another
variant of this approach would be to benchmark pre-
mium subsidies to a plan with generous benets, similar
to the Medicare program or a gold plan under cur-
rent law. Under this approach, people would use their
subsidy to purchase a plan of their choice from a health
insurance marketplace that included multiple private
26. First-dollar cost sharing is the amount that an enrollee is required
to pay out of pocket before the health plan starts to pay for
benets.
27. See Ed Dolan, Universal Catastrophic Coverage: Principles for
Bipartisan Health Care Reform (Niskanen Center, June 2019),
https://tinyurl.com/y4jkfzco (PDF, 969 KB). See also Dana
Goldman and Kip Hagopian, “e Health-Insurance Solution,”
National Aairs (Fall 2012), https://tinyurl.com/y3es67tp.
plans.
28
A public option also could be oered alongside
private plans, similar to the current Medicare program,
which gives people the choice of enrolling in traditional
Medicare or a Medicare Advantage plan.
29
An approach
that oered fully subsidized generous coverage would
require more federal spending than an approach that
oered fully subsidized catastrophic coverage.
Approach 4: A Single-Payer System
Under a single-payer system, everyone in the dened
population would receive health insurance coverage from
the same public plan, and there generally would be no
role for private insurance. ere would be no premiums,
and to achieve decit neutrality, such a system would
need to be nanced through broad-based tax revenues;
that is, new mechanisms of nancing also would be
required.
30
is approach would involve the most sig-
nicant departure from the current health care system,
and it would be an enormously complex undertaking.
Under current law, people receive coverage through
various public and private sources, as described earlier in
this report. Under a single-payer system, there generally
would be no role for employment-based insurance, and
the role of other public programs, such as Medicaid and
Medicare, would be greatly reduced or eliminated.
Enrollment Process. Under a single-payer system, the
government would strive to enroll all people in the
dened population in the public plan. People also could
be automatically enrolled at the time they were issued
Social Security numbers, newborns could be enrolled
in hospitals, and other eligible people could be enrolled
at the time they sought medical care. Some people
seeking medical care would not be eligible for enroll-
ment—because they were visiting from another country,
28. See George Halvorson and Mehmet Oz, “Medicare Advantage for
All Can Save Our Healthcare System,” Forbes (June 11, 2020),
https://tinyurl.com/yyjvw8j2.
29. See Billy Wynne, “e Bipartisan ‘Single Payer’ Solution:
Medicare Advantage Premium Support for All,” Health Aairs
Blog (May 2017), https://tinyurl.com/y6xba4hx; Georey
Joyce, “Opinion: e Success of Medicare Advantage Makes It
a Better Policy Choice an ‘Medicare for All,’” MarketWatch
(November 21, 2019), https://tinyurl.com/y42cj4z; and Ken
Janda and Vivian Ho, “Medicare Advantage for All,” e Hill
(August 27, 2019), https://tinyurl.com/y6avusv8.
30. For further details, see Congressional Budget Oce, Key
Design Components and Considerations for Establishing a
Single-Payer Health Care System (May 2019), www.cbo.gov/
publication/55150.

32 Policies to Achieve NeAr-UNiversAl heAlth iNsUrANce coverAge october 2020
for instance—and the enrollment system would need
to conrm that they were not eligible. Because people
would need to provide information to the enrollment
system and some would not do so, coverage would not
be completely universal.
Premiums. ere would be no premiums under a
single-payer system. To achieve decit neutrality, such a
system would need to be nanced through broad-based
tax revenues.
Cost Sharing and Benets. A single-payer system would
have lower cost sharing than the average under current
law. Such a system could include no cost sharing for
most services. If the single-payer system included cost
sharing, there could be exceptions for certain popula-
tions, such as people with low income, children, and the
disabled.
e single-payer system would provide comprehensive
major medical coverage, but certain items and services,
such as over-the-counter medications and cosmetic
procedures, could be excluded from coverage. Existing
proposals cover a more comprehensive set of benets
than many current sources of coverage, including dental,
vision, hearing, and long-term services and supports, but
a single-payer system could be designed without those
additional benets.
Role of Private Plans. ere generally would be no role,
or a very limited role, for private insurance. If private
insurance was allowed, it could be limited to services not
covered by the public plan. However, private insurance
also could be oered as an alternative source of coverage
if enrollees and providers were allowed to opt out of the
single-payer system. Alternatively, private insurance could
provide benet enhancements, such as faster access to
care or private rooms instead of semiprivate rooms for
inpatient stays, or it could be used to access providers that
opt out of the single-payer system or to seek care abroad.
Role of Employment-Based Insurance. Employment-
based insurance probably would no longer exist under a
single-payer health system, or its role would be greatly
reduced. For instance, it might provide supplemental
coverage for services not covered by the public plan or
reduce cost-sharing amounts, if any.
Role of Public Programs. Most public programs, such as
Medicaid, CHIP, and Medicare probably would have a
limited role or be eliminated under a single-payer system.
Some components of those programs could continue to
operate separately and provide benets for services not
covered by the single-payer health plan. For example,
Medicaid and CHIP could continue to provide long-term
services and support benets only to low-income popula-
tions, but the Medicare program would no longer exist.
Examples of is Approach. e two versions of the
Medicare for All Act of 2019include many of the fea-
tures described in this approach, including no premiums,
comprehensive major medical coverage, limited to no
cost sharing, and no private insurance that would dupli-
cate the benets of the single-payer system.
31
31. See the Medicare for All Act of 2019, H.R. 1384 and S. 1129,
116th Cong.

List of Tables and Figures
Tables
1. Summary of Approaches to Achieve Near-Universal Health Insurance
Coverage rough a Default Plan 4
2. Key Features of Approaches to Achieve Near-Universal Health Insurance
Coverage rough a Default Plan Compared With the System in Eect Under Current Law 5
Figure
1. Eligibility for Subsidized Coverage Among Uninsured People in 2019 10

About This Document
is report was prepared at the request of Chairman John Yarmuth of the House Committee on
the Budget and Representatives Angie Craig, Lizzie Fletcher, and Susan Wild. In keeping with the
Congressional Budget Oce’s mandate to provide objective, impartial analysis, the report makes
no recommendations.
Jared Maeda and Karen Stockley wrote the report with guidance from Chapin White
and Jerey Kling. Caroline Hanson, Grace Hwang, Sarah Masi, John McClelland,
Alexandra Minicozzi, Lyle Nelson, and Julie Topoleski provided useful comments.
Christian Henry and Rachel Matthews fact-checked the report.
Edwin Dolan of the Niskanen Center, Matthew Fiedler of the Brookings Institution,
Glenn Hubbard of Columbia University, Topher Spiro of the Center for American Progress, and
Gail Wilensky of Project Hope provided helpful comments. e assistance of external reviewers
implies no responsibility for the nal product, which rests solely with CBO.
Robert Sunshine reviewed the report. Loretta Lettner was the editor, and Casey Labrack
was the graphics editor. An electronic version is available on CBO’s website (www.cbo.gov/
publication/56620).
CBO continually seeks feedback to make its work as useful as possible. Please send any comments
to [email protected]v.
Phillip L. Swagel
Director
October 2020
